INTRODUCTION
Vedolizumab (VDZ) is an anti-╬▒4╬▓7 integrin antibody and has a well-established efficacy in inflammatory bowel diseases (IBD), including ulcerative colitis (UC) and CrohnŌĆÖs disease (CD). Notably, because of its unique mechanism of inhibiting the migration of immunocompetent cells to the intestinal tract, it has a favorable safety profile and the risk of opportunistic infections is low [1,2]. Real-world data has also reported the safety of VDZ, with the lowest risk of opportunistic infections when it is used as a single agent [3]. Although there are few reports on direct comparison with other advanced therapies, alternative network meta-analyses have shown that VDZ has the highest safety profile (especially for UC) [4,5]. An elective switch from anti-tumor necrosis factor (TNF) agents to VDZ due to reasons other than loss of response has been reported in patients maintaining clinical remission on anti-TNF agents, with an observed VDZ-maintained clinical remission rate of 82.9% during a median duration of 30 months [6]. Such an elective switch may be a useful option for patients with safety concerns, but not with high disease activity.
In immunocompromised patients, viral infections such as measles, mumps, rubella, and varicella can be severe or life threatening. Patients with IBD receiving immunosuppressive therapy may have low antibody titers to these viruses, and there are a certain number of IBD patients with negative antibody titers [7,8]. Therefore, in countries such as Japan that have inadequate public vaccination programs for these viruses [9,10] and in other developed countries where sporadic outbreaks due to vaccine refusal have been observed [11,12], appropriate vaccination is required in patients without verified vaccination or with negative antibody titers. Furthermore, vaccination coverage has declined worldwide during the coronavirus disease 2019 (COVID-19) pandemic, which has raised concerns about vaccine-preventable disease outbreaks [13,14]. However, unlike inactivated vaccines, live-attenuated vaccines against measles, rubella, mumps, and varicella viruses are contraindicated for patients on immunosuppressive therapy [15-17].
Live-attenuated vaccination is contraindicated for approximately 4 weeks prior to initiating or 3 months after discontinuing immunosuppressive agents [15-20]. Ideally, live-attenuated vaccines should be administered at the time of diagnosis or prior to the initiation of immunosuppressive therapy; however, in practice, there may be insufficient time for vaccination due to disease severity. After starting immunosuppressive therapy, drug cessation for vaccination may result in an increased risk of disease flare. Among immunosuppressive agents, VDZ is a gut-selective agent and is expected to have little systemic effects. For IBD patients treated with other advanced therapies, switching to VDZ and subsequently receiving live-attenuated vaccination may minimize the risk of both vaccine-related viral infection and relapse of IBD, except for vaccination against gastrointestinal pathogens such as rotavirus. The package inserts for VDZ states that patients on this agent may receive a live vaccine if the benefits outweigh the risks [17]. However, only 1 case has been reported in which a measles vaccine was administered while continuing VDZ, with no adverse events during the 3-month follow-up period [21].
To develop an appropriate vaccination strategy among IBD patients under immunosuppressive therapy, we aimed to assess the feasibility of live-attenuated vaccination while continuing VDZ and switching from other advanced therapies to VDZ and subsequent live-attenuated vaccination.
METHODS
1. Selection of Eligible Cases
In our previous study, we measured antibody titers specific for measles, rubella, mumps, and varicella viruses in patients aged 16 or older and with a confirmed diagnosis of CD or UC at our university hospital [8]. The diagnosis of CD or UC was based on the diagnostic criteria proposed by the Research Group of Intractable Inflammatory Bowel Disease under the guidance of the Ministry of Health, Labour, and Welfare of Japan [22,23]. Regarding medical treatments, only patients receiving advanced therapies (infliximab [IFX], adalimumab [ADA], golimumab [GLM], ustekinumab [UST], VDZ, or tofacitinib) and/or thiopurines (azathioprine or 6-mercaptopurine) between March 2020 and May 2023 were included.
Using enzyme-linked immunosorbent assays (SRL Inc., Tokyo, Japan), specific IgG titers of < 2.0, 2.0-4.0, and > 4.0 IU/mL were considered seronegative, equivocal, and seropositive, respectively [8]. Considering the childhood immunization schedule in Japan [8,20], patients with negative antibody titers and without a verified vaccination history were judged to be unimmunized. Even in cases with negative or equivocal immunity, certification of recommended childhood vaccinations was sufficient to be considered immunized [18]. Therefore, cases with well-documented vaccination history were excluded from this study. Unlike measles and rubella, protection against mumps may not be as durable [24]; therefore, patients unimmunized only for mumps were also excluded.
To assess disease activity, CrohnŌĆÖs Disease Activity Index (CDAI) or partial Mayo score (Mayo score excluding endoscopic subscore) were used in patients with CD or UC, respectively. Remission was defined as a CDAI of less than 150 or a partial Mayo score of 0 or 1, and mild severity as a CDAI of 150-219 or a partial Mayo score of 2-4. Recurrence was defined as an increase of 70 or more in CDAI or an increase of 2 or more in partial Mayo score. Since there is no convincing evidence that the severity of IBD will be exacerbated by vaccination [17,18], we were not concerned about the severity at the time of vaccination. However, because of safety concerns, patients with moderate to severe disease severity were excluded from this study.
The Ethics Committee of Tohoku University Hospital approved the study protocol on 17 March 2020 (No. 18388). All participants provided written informed consent. This study was registered with the University Hospital Medical Information Network Center Trials registry, UMIN000034662.
2. Procedure of Vaccination
In patients unimmunized against measles, mumps, rubella, or varicella viruses and with quiescent or mild disease severity, live-attenuated vaccines were administered in when the benefits of vaccination exceed the risks. If the patient had been treated with VDZ, live-attenuated vaccines were administered while continuing VDZ. By contrast, if the patient had been treated with a different biological agent, the agent was switched to VDZ after careful consideration of the risks of disease relapse. After at least 3 months, live-attenuated vaccines were then administered. In both cases, patients were involved in the decision-making process regarding vaccination and drug switching. To further reduce the risk of vaccination, thiopurines were also discontinued after discussion with the patient. According to the recommended vaccination schedule [15,17,20], if the patient had a history of childhood vaccination at 1 year of age or older, he or she was vaccinated once. If no history of childhood vaccination could be confirmed, he or she was vaccinated twice with an interval of at least 4 weeks. Antibody titers were remeasured at least 4 weeks after the last vaccination. During these procedures, disease progression and severity were carefully monitored.
The live-attenuated vaccines used in the present study were as follows: dried live-attenuated measles and rubella combined vaccine, Mearubik (Tanabe strain and Matsuura strain; Mitsubishi Tanabe Pharma Co., Osaka, Japan), dried live-attenuated mumps vaccine (Torii strain; Takeda Pharmaceutical Co., Ltd., Osaka, Japan) and dried live-attenuated varicella vaccine (Oka strain, Takeda Pharmaceutical Co., Ltd.).
3. Primary and Secondary Outcomes
The rate of patients maintaining disease severity without recurrence 8 weeks after live-attenuated vaccination and the rate of patients without vaccine-induced infection during the 2-year follow-up period were defined as the co-primary outcomes. Seropositive rate of measles, mumps, rubella, or varicella was defined as secondary outcome. In patients who switched their biological agent from another to VDZ, the rate of patients maintaining disease severity 54 weeks after switching to VDZ was also defined as the secondary outcome.
4. Statistical Analysis
Data are presented as the median and interquartile range (IQR; first to third quartile). Using the chi-square test, Fisher exact probability test or Wilcoxon signed-rank test, we assessed differences between the groups, as appropriate. These analyses were performed using the JMP Pro version 16 software program (SAS Institute Inc.; Cary, NC, USA). P<0.05 indicated a statistically significant difference.
RESULTS
1. Clinical Characteristics and Medical Treatments
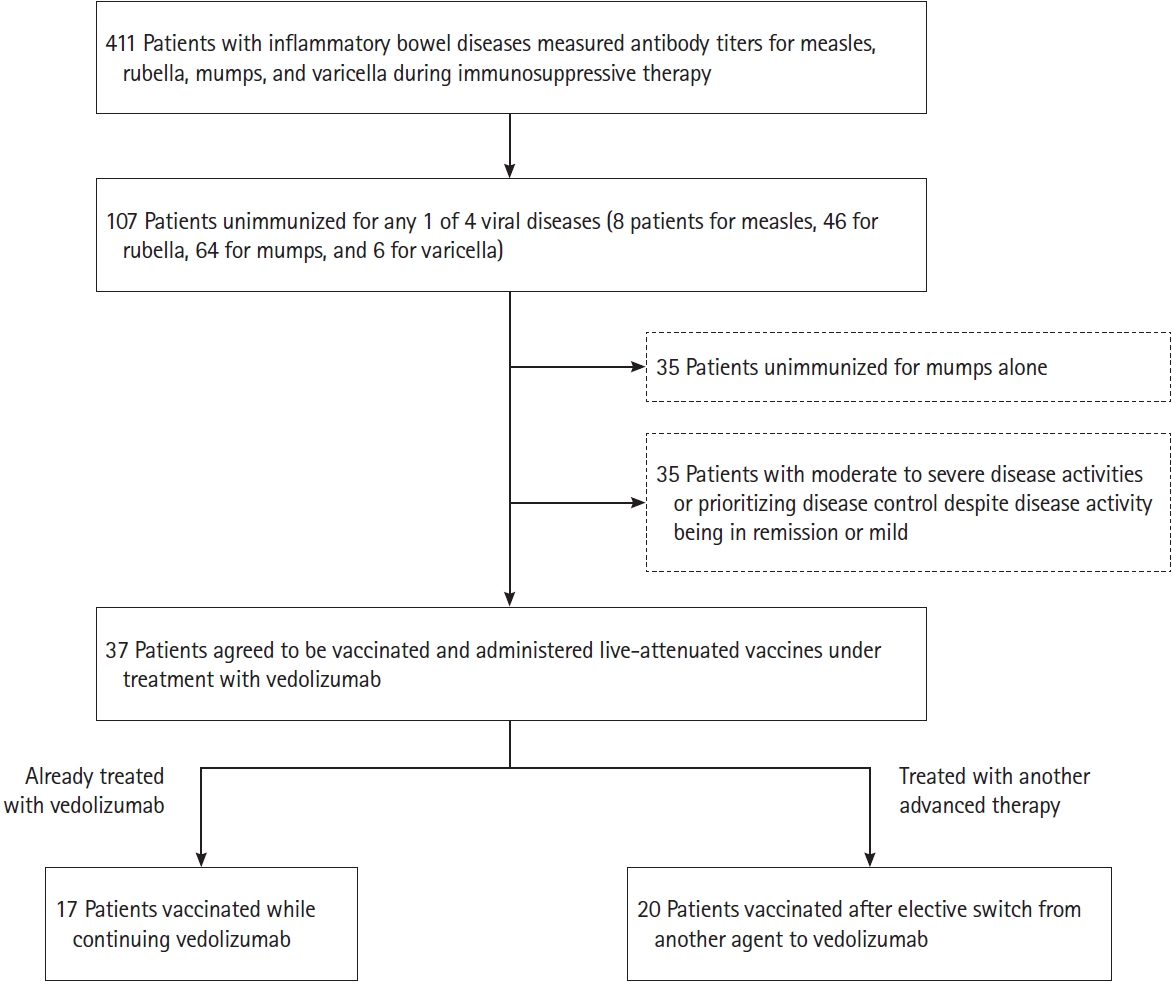
Among 411 patients with IBD whose antibody titers were measured during immunosuppressive therapy in our previous study [8], 8 patients were determined to be unimmunized for measles, 46 for rubella, 64 for mumps, and 6 for varicella. A total of 107 patients were determined to be unimmunized for any 1 of the 4 viral diseases. Of these 107 patients, 35 patients unimmunized for mumps alone were excluded. After explaining the risks and benefits of vaccination, 35 patients were also excluded because they had moderate to severe disease severity or they prioritized the control of their disease even if their disease were in remission or only mildly severe. Finally, 37 patients agreed to be vaccinated while continuing VDZ (17 patients) or after elective switch from another advanced therapy to VDZ (20 patients) (Fig. 1).
The clinical characteristics of these 37 patients are shown in Table 1. They consisted of 29 males (78.4%) and 8 females (21.6%); 23 patients had CD, while 14 patients had UC. The median age at diagnosis, the median age at enrollment, and the median disease duration were 23 years (IQR, 20.0-29.0 years), 33 years (23.5-38.5 years), and 6 years (0.5-10.0 years), respectively. In patients with CD, the disease location was divided into ileitis (n = 6, 26.1%), ileocolitis (n = 12, 52.2%), and colitis (n = 5, 21.7%). In UC patients, the disease extent was divided into total colitis (n = 9, 64.3%) and left-sided colitis (n = 5, 35.7%). In patients with CD, anal lesions were seen in 16 patients (69.6%), while 10 patients (43.5%) had 1 or more surgeries for CD.
Regarding immunosuppressive therapy, 10 patients were managed with IFX, 7 with ADA, 1 with GLM, 2 with UST, and 17 with VDZ. Seventeen of the 37 patients were treated in combination with thiopurines (12 with azathioprine and 5 with 6-mercaptopurine). There were no differences in clinical characteristics between patients who agreed to be vaccinated and those who declined.
2. Elective Switch from Another Advanced Therapy to VDZ
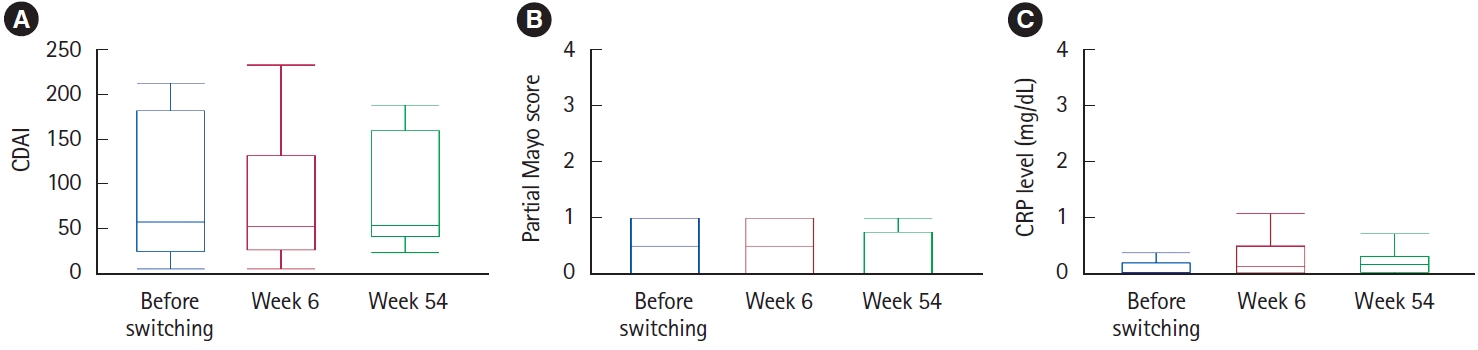
The treatment was changed from another advanced therapy to VDZ in 20 patients in remission or mild disease severity. Median duration of advanced therapy prior to switching to VDZ was 77.5 months (37.5-99.5 months). In 16 CD patients switched to VDZ, CDAI was maintained from a median of 56 (IQR, 23-180) at the time of switching to 51 (25-130, P=0.50) at 6 weeks and 52 (40-158, P=0.84) at 54 weeks (Fig. 2A). In 4 UC patients switched to VDZ, the partial Mayo score also remained from a median of 0.5 (IQR, 0-1) at the time of switching to 0.5 (0-1, P=1.00) at 6 weeks and 0 (0-1, P=1.00) at 54 weeks (Fig. 2B). The changes in C-reactive protein (CRP) levels in all 20 patients are shown in Fig. 2C. CRP levels slightly increased from a median of 0.04 (IQR, 0.02-0.19) at the time of switching to 0.14 (0.02-0.50, P=0.004) at 6 weeks and 0.16 (0.03-0.31, P=0.002) at 54 weeks, including 1 CD patient who developed an intestinal infection as a possible cause.
Within 54 weeks from switching to VDZ, 2 patients (ileocolitis CD and colitis CD) had moderate relapses and switched to their original advanced therapies (both to ADA). After 54 to 102 weeks, 2 patients (ileocolitis CD and total colitis UC) had mild relapses and switched to their original advanced therapies (one to UST, the other to ADA). One patient developed ileus due to a long-identified ileal stricture and was switched to UST after ileocecal resection. In all 5 cases, vaccination was completed prior to treatment alteration, and disease activity subsided after treatment alteration. None of the cases required re-administration of thiopurines.
3. Vaccination and Subsequent Change in Disease Severity
A total of 37 patients (17 remaining on VDZ and 20 switched to VDZ) received live-attenuated vaccines. The measles and rubella combined vaccine was administered to 30 patients, the rubella vaccine to 2 patients, the mumps vaccine to 18 patients, and the varicella vaccine to 2 patients (with some overlapping). When 2 doses of the same vaccine were given, the second vaccine was administered at least 4 weeks apart. Prior to vaccination, thiopurines were also discontinued except for 2 patients who preferred to continue them.
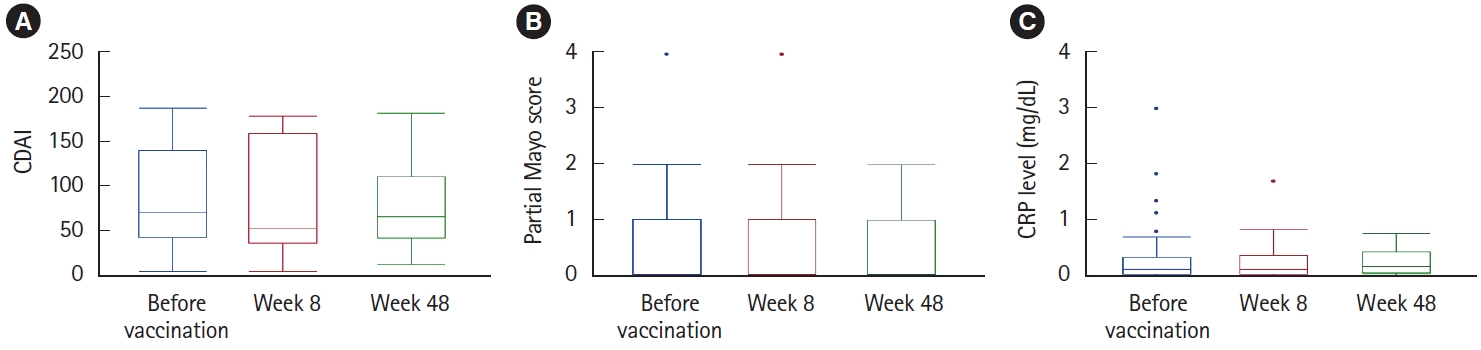
In 23 vaccinated patients with CD, CDAI was maintained from a median of 69.5 (IQR, 42-139) at the time of vaccination to 52 (36-157, P=0.60) at 8 weeks and 65 (42-109, P=0.31) at 48 weeks (Fig. 3A). In 14 vaccinated patients with UC, the partial Mayo score also remained from a median of 0 (IQR, 0-1) at the time of vaccination to 0 (0-1, P=1.00) at 8 weeks and 0 (0-1, P=1.00) at 48 weeks (Fig. 3B). According to the aforementioned definition, there were no cases of relapse with an increase of more than 70 in CDAI or an increase of more than 2 in Partial Mayo score at 8 weeks. The CRP levels in all 37 vaccinated patients are shown in Fig. 3C, which were maintained from a median of 0.11 (IQR, 0.03-0.33) at the time of vaccination to 0.11 (0.04-0.36, P=0.84) at 8 weeks and then slightly increased to 0.16 (0.05-0.42, P=0.002) at 48 weeks.
Antibody titers were remeasured at least 4 weeks after the last vaccination. In vaccinated cases, antibody titers against measles, rubella, mumps, and varicella increased from 3.4 (2.0-18.0) to 7.8 (4.8-24.6) IU/mL, from 1.4 (0.5-3.8) to 5.9 (2.5-12.6) IU/mL, from 1.7 (1.2-2.4) to 4.2 (3.2-5.1) IU/mL, and from 1.9 (1.7-2.2) to 2.9 (2.8-5.8) IU/mL, respectively. As a result, antibody titers changed to positive or equivocal in 34 patients (91.9%), including 5 patients who required treatment alterations a while after the completion of vaccination. While, only antibody titers against rubella remained negative in 3 CD patients. Among the 3 patients, 2 were simultaneously vaccinated against measles (the measles and rubella combined vaccine) and the other against mumps. Antibody titers against measles changed from negative to equal in 1 case and remained equal in the other. Antibody titer against mumps changed from negative to positive. There were no cases of vaccine-induced infection or vaccine-related adverse events during a median observation period of 121 weeks (88-143 weeks).
DISCUSSION
Because VDZ is a gut-selective agent, it has a weak systemic immunosuppressive effect and has been demonstrated to have a favorable safety profile [1-5]. For patients with severe or perianal disease, other advanced therapies, such as anti-TNF agents, may be preferable. However, especially when a patient may be exposed to other infectious diseases, e.g., during the COVID-19 pandemic, it may be acceptable to switch from other advanced therapies to VDZ if the patient is in remission or has mild disease severity. In the present study, of the 20 patients who electively switched from another biological agent to VDZ, only 1 experienced temporary flare up due to intestinal infection. Furthermore, within 1 year from switching to VDZ, only 2 patients reverted to their original biological agent because of relapse. In patients with several comorbidities who choose another advanced therapy due to their disease severity, it may be acceptable to switch to VDZ once their disease is under control.
Live-attenuated vaccines against measles, rubella, mumps, or varicella viruses are contraindicated under immunosuppressive therapy, especially under biologic therapy [15-20]. In a previous review [25], the safety of live-attenuated vaccination under immunosuppressive therapy was assessed in 20,556 patients with immune-mediated inflammatory diseases, including 2,852 IBD patients. Of these 20,556 patients, 474 received measles, mumps, and rubella (MMR) vaccination, and only 1 vaccine-induced infection was seen [25]. While this review demonstrated the safety of live-attenuated vaccines administration, the number of patients treated with advanced therapies was extremely low.
Different from other advanced therapies, VDZ is amongst the lowest risk immunosuppressive therapies along with 5-aminosalicylic acid, low-dose corticosteroids, and budesonide [26]. Although the package insert for VDZ states that patients may receive live-attenuated vaccines if the benefits outweigh the risks [17], the safety of live-attenuated vaccination under VDZ therapy has not been fully evaluated. In the present study, live-attenuated vaccines against measles, rubella, mumps, or varicella viruses were administered to 37 patients receiving VDZ (17 remaining on VDZ and 20 switched to VDZ). As stated in the Canadian guidelines [19], there is sparse data on MMR vaccine administered outside the standard childhood schedule. However, most patients acquired immunity after vaccination, and none showed vaccine-related viral infection. Particularly for patients treated with another advanced therapy, switching to VDZ and subsequently receiving vaccination may also be a safe alternative to minimize the risk of vaccine-related viral infection and disease progression.
In addition, VDZ has shown more favorable immunogenicity to vaccination compared to other agents such as anti-TNF and Janus kinase inhibitors [27-29].
In Asian countries including Japan, inadequate public vaccination programs have led to insufficient control of infection among measles, rubella, mumps, and varicella [9,10]. The presence of IBD may also result in lower seropositivity rates for these viruses [24,30,31]. We also reported that seropositive rates for these viruses in IBD patients under immunosuppressive therapy were lower than those in gender- and age-matched healthy subjects living in the same area [8]. Even in Western countries where public vaccination programs have been thoroughly implemented, global outbreaks of measles have been reported partly due to so-called ŌĆ£vaccine hesitancyŌĆØ [11,12] and the COVID-19 pandemic [13,14]. It is important to measure viral antibody titers and vaccinate if necessary prior to initiating immunosuppressive therapy [16-20]. However, even if antibody titers are measured prior to therapeutic intervention, most cases with moderate to severe disease do not allow sufficient time for vaccination. Our current study provides a possible solution of how to administer live-attenuated vaccines for those with negative antibody titers under immunosuppressive therapy by switching to VDZ treatment once disease activity is under control.
In contrast to live-attenuated measles, rubella, and mumps vaccines, a recombinant (inactivated) subunit vaccine for herpes zoster has become available. With its safety and efficacy in IBD patients gradually being reported, there may be an advantage for immunosuppressed IBD patients [32,33]. Notably, this subunit vaccine can only be used to prevent herpes zoster (shingles), but not varicella (chicken pox). Varicella under immunosuppressive therapy is a rare but life-threatening disease as shown that 5 out of 20 IBD patients infected with varicella have died [34].
This study has several limitations. First, this study only includes a small number of cases. Since the number of patients with both negative antibody titers and low disease activity was limited, it is difficult to overcome this small sample size. Future larger studies are required to validate the efficacy and safety of live-attenuated vaccination under VDZ therapy. By contrast, a median follow-up period of about 2 years may be sufficient to address the advantages or disadvantages of elective switch from other advanced therapies to VDZ followed by live-attenuated vaccination. Second, we did not perform an endoscopic examination or measure fecal calprotectin, a surrogate marker of endoscopy, to accurately assess IBD disease severity. Although the severity of the disease may need to be judged more carefully, especially when making a drug switch to VDZ, the majority of the present cases were in clinical remission for a long period of time. Also, cases categorized as mild severity because of high stool frequency were in biochemical remission if based on CRP. To reduce patient burden, endoscopic examination is not routinely performed.
Patients receiving immunosuppressive therapy are at greater risk of developing a variety of infectious diseases. Therefore, minimizing the risk of developing vaccine-preventable infections should be important for patient care and management. Our study suggests that live-attenuated vaccine may be safely administered under VDZ therapy. Switching from another advanced therapy to VDZ and subsequently receiving vaccines may be a safe alternative to reduce the risk of vaccine-induced infection and relapse of IBD.