INTRODUCTION
Coronavirus disease (COVID-19) is an infectious disease caused by the novel coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; formerly called 2019-nCoV) and was first identified in Wuhan, China. Globally, as of October 18, 2022, there have been 622,389,418 confirmed COVID-19 cases, including 6,548,492 deaths, reported to the World Health Organization (WHO) [1].
Since the onset of the COVID-19 pandemic, various types of vaccines have been developed to prevent the spread of COVID-19 worldwide [2]. According to recent large-scale studies, vaccination has been effective in reducing hospitalizations, progression to severe disease, and deaths [3]. Moreover, it has been effective in preventing both asymptomatic and symptomatic infections [3]. However, as patients with inflammatory bowel disease (IBD) have been excluded from large-scale clinical studies on COVID-19 vaccines, the impact of vaccination on IBD patients is still unknown.
As IBD is a chronic inflammatory immune-mediated intestinal disease, there have been concerns that vaccination might impair the immune system of the intestinal mucosa, leading to an IBD flare. Prior studies have assessed the exacerbation of IBD after vaccination against various pathogens, such as influenza, zoster, and pneumococcus, but there is no evidence that these vaccinations induce IBD flares [4-6]. However, little is known about whether COVID-19 vaccination affects the exacerbation of IBD.
Patient-reported outcomes (PROs) have been increasingly regarded as crucial outcome measures in IBD-related studies, with the recent recognition of the importance of direct impacts on patients, beyond its effects on disease activity [7]. PROs emphasize the experiences that patients had with the disease, including thoughts, impressions, perceptions, and attitudes [8]. With the recent development of guidelines for the Food and Drug Administration (FDA) PROs, greater attention is being paid to the role and importance of PRO in healthcare [9]. However, there have been no studies assessing changes in PROs after vaccination in patients with IBD.
Therefore, in this study, we investigated the impact of COVID-19 vaccines on the PROs of patients with IBD.
METHODS
1. Patients
We conducted a questionnaire survey of patients with IBD who visited 4 specialized outpatient IBD clinics of referral university hospitals from April 2022 to June 2022. Patients who were previously diagnosed with IBD by gastroenterologists at these hospitals and currently undergoing outpatient follow-up observations, were older than 18 years of age, had received at least one dose of COVID-19 vaccination between March 2021 and June 2022, and were clinically inactive for IBD were included in this study. Clinically inactive was defined as no change in medication, including the dose for IBD treatment, without complaints of distinct symptoms within 1 year before the first vaccination [10,11].
We excluded patients who had intestinal Beh├¦etŌĆÖs disease, ulcerative colitis (UC) with a partial Mayo score (pMayo) Ōēź 5, or CrohnŌĆÖs disease (CD) with a CrohnŌĆÖs Disease Activity Index (CDAI) Ōēź 220. A survey was conducted with 320 patients, and 11 patients were excluded according to the above criteria. Finally, a total of 309 patients were enrolled in this study (Fig. 1).
The study protocol was approved by the institutional review of each participating center, including Severance Hospital (IRB No. 4-2021-1062), Asan Medical Center (IRB No. 2021-1872), and Daejeon St. Mary's Hospital (IRB No. DC22QIDI0024), and conformed to the ethical guidelines of the 1975 Helsinki Declaration. All study participants provided written informed consent prior to study enrollment.
2. Variables from the Survey and Medical Records
The following information was collected from the questionnaire: age, sex, IBD type, smoking history, family history, COVID-19 vaccination history, COVID-19 infection history, adverse events after vaccination, self-imposed cessation of IBD medications, and scores of PROs. Family history ascertained whether the patients with IBD had first-degree relatives who had IBD. The COVID-19 vaccination history included the type of vaccination by order and date of vaccination. Self-imposed cessation of IBD medications was defined as the cessation of IBD-related medications owing to adverse events after vaccination, although the drug was not discontinued. The following PROs were investigated: UC PROs signs and symptoms (UC-PRO/SS), CD PROs signs and symptoms (CD-PRO/SS), and the short health scale (SHS). Each PRO was obtained within 3 months before the first dose of the vaccine and within 3 months after each dose.
The patients were vaccinated with 5 types of vaccines. The AstraZeneca, Janssen, and Novavax vaccines are viral vector vaccines that are similar to conventional viral vaccines. Moderna and Pfizer are new types of mRNA vaccines. All the 5 vaccines were inactivated.
The following medical records were obtained within 3 months prior to the first dose of the vaccine and within 3 months after each dose: the degree of physiciansŌĆÖ global assessment, CDAI scores for CD patients, pMayo scores for UC patients, levels of hemoglobin, white blood cell count, lymphocyte count, platelet count, albumin, C-reactive protein, fecal calprotectin, and platelet-to-lymphocyte ratio.
3. Patient-Reported Outcomes
UC-PRO/SS, CD-PRO/SS were developed to standardize the quantification of gastrointestinal signs and symptoms in patients with UC and CD using direct reports from patient ratings. These are the first symptom measures of UC and CD to meet the U.S. FDA PRO guidelines [12,13]. The UC-PRO/SS measure includes 2 scales: bowel signs and symptoms (UC-PRO/ SS(B), range: 0-28), which includes 6 items; and abdominal symptoms (UC-PRO/SS(A), range: 0-12), which includes 3 items, each scored separately [12]. The CD-PRO/SS measure includes 2 scales: bowel signs and symptoms (CD-PRO/SS(B), range: 0-16), which includes 3 items; and abdominal symptoms (CD-PRO/SS(A), range: 0-12), which includes 3 items, each scored separately [13]. Each scale of UC and CD showed evidence of adequate reliability, reproducibility, and validity, including moderate-to-high correlations with the pMayo and Inflammatory Bowel Disease Questionnaire score for UC and moderate correlations with the Inflammatory Bowel Disease Questionnaire score for CD [12,13].
In this study, the primary endpoint was an increase in PRO scores after COVID-19 vaccination. This was defined as an increase by 4 or more in the UC-PRO/SS or the CD-PRO/SS scores after vaccination when compared to the baseline.
SHS is a simple, 4-part visual analog scale questionnaire designed to assess the impact of IBD on health-related quality of life [14,15]. The 4 dimensions include symptom burden, social function, disease-related worry, and sense of general well-being. The scores for each dimension range from 0 to 100 [14,15]. In previous studies, patients with IBD in relapse scored higher on each of the 4 SHS questions than patients in remission. Each of the 4 SHS scores was associated with the results of their corresponding health dimension obtained with the other health-related quality of life questionnaires [16,17]. This score was validated in different languages for a variety of IBD patients [16-18].
4. Statistical Analysis
All numerical values are expressed as means ┬▒ standard deviations or numbers (percentages). Continuous variables were compared using the Student t-test or Mann-Whitney U-test, and categorical variables were compared using the chi-square test or Fisher exact test. Risk factors associated with an increase in PROs after COVID-19 vaccination in each patient group for IBD, UC, and CD were analyzed using logistic regression analysis. Odds ratios (OR) and 95% confidence intervals (CI) were calculated to estimate the effects of variables. In addition, we assessed whether there were differences in variables by vaccine order using multiple pairwise comparisons, especially the linear mixed model. Bonferroni correction was used to avoid the possibility of obtaining false positive results. Statistical significance was set at P< 0.05. All statistical analyses were performed using IBM SPSS Statistics version 28.0 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Baseline Characteristics
The baseline characteristics of the patients are summarized in Table 1. In total, 47.9% (n = 148) of patients had UC and 52.1% (n = 161) had CD. The mean patient age was 40.8 years, and 64.4% (n = 199) of the patients were male. Seven point eight percent of the patients had a smoking history, and 31.0% had a family history.
All the patients included in this study received their first vaccination: 64.1% with Pfizer (n = 198); 17.2% with Moderna (n = 53); 15.9% with AstraZeneca (n = 49); 2.6% with Janssen (n = 8), and 0.3% with Novavax (n = 1). A total of 307 (99.4%) patients received a second vaccine: 69.4% with Pfizer (n = 213), 18.2% with Moderna (n = 56), 10.4% with AstraZeneca (n = 32), 1.6% with Janssen (n = 5), and 0.3% with Novavax (n = 1). A total of 251 (81.2%) patients received a booster vaccine: 72.1% with Pfizer (n = 181), 26.7% with Moderna (n = 67), 0.8% with AstraZeneca (n = 2) and 0.4% with Novavax (n = 1). The number of patients with a history of COVID-19 was 121 (39.2%). Although the medications should not be discontinued, the proportion of patients who self-suspended IBD-related medications owing to adverse effects after vaccination was 8.8% (n = 27). The baseline means were as follows: SHS was 7.36 ┬▒ 7.08, CD-PRO/SS(A) was 3.01 ┬▒ 2.40, UC-PRO/SS(A) was 2.05 ┬▒ 1.97, CD-PRO/SS(B) was 3.01 ┬▒ 2.40, and UC-PRO/SS(B) was 4.57 ┬▒ 3.21. The mean pMayo score of patients with UC was 0.94 ┬▒ 0.94, and the mean CDAI score of patients with CD was 74.04 ┬▒ 52.52.
2. Adverse Events after Vaccination
The characteristics of the adverse events after vaccination are summarized in Tables 2 and 3. After vaccination, the proportion of patients who experienced adverse events was 78.3% (n = 242/309), 80.1% (n = 246/307), and 74.5% (n = 187/251) after the 1st, 2nd, and 3rd inoculation, respectively. The most common adverse events after vaccination were injection site pain and redness (1st, 47.6%; 2nd, 45.0%; 3rd, 40.6%), fatigue (1st, 34.3%; 2nd, 31.9%; 3rd, 27.9%), fever (1st, 25.0%; 2nd, 21.5%; 3rd, 19.9%), and general myalgia (1st, 21.7%; 2nd, 16.9%; 3rd, 19.1%). Anaphylaxis occurred twice in 1 patient after receiving AstraZeneca as the second vaccine and Pfizer as the third vaccine, and there were no deaths after vaccination.
3. Risk Factors Related to the Aggravation of PROs after Vaccination
We compared groups with and without aggravation of PROs after vaccination using univariate analysis (Tables 3-5). In all patients, age and platelet count were significantly associated with aggravation of PROs (Table 3). In addition, age, platelet count, and platelet-to-lymphocyte ratio significantly aggravated PROs in UC patients (Table 4). In contrast, risk factors that aggravated PROs were not found in the univariate analysis in CD patients (Table 5).
The independent risk factors, for the aggravation of PROs, in the multivariate analysis were: young age (less than 40 years) (OR, 4.255; 95% CI, 1.816-9.968) and UC (OR, 2.654; 95% CI, 1.216-5.794) in patients with IBD, young age (OR, 8.667; 95% CI, 2.062-36.425) in patients with UC, and male sex in patients with CD (OR, 4.103; 95% CI, 1.115-15.104) (Table 6).
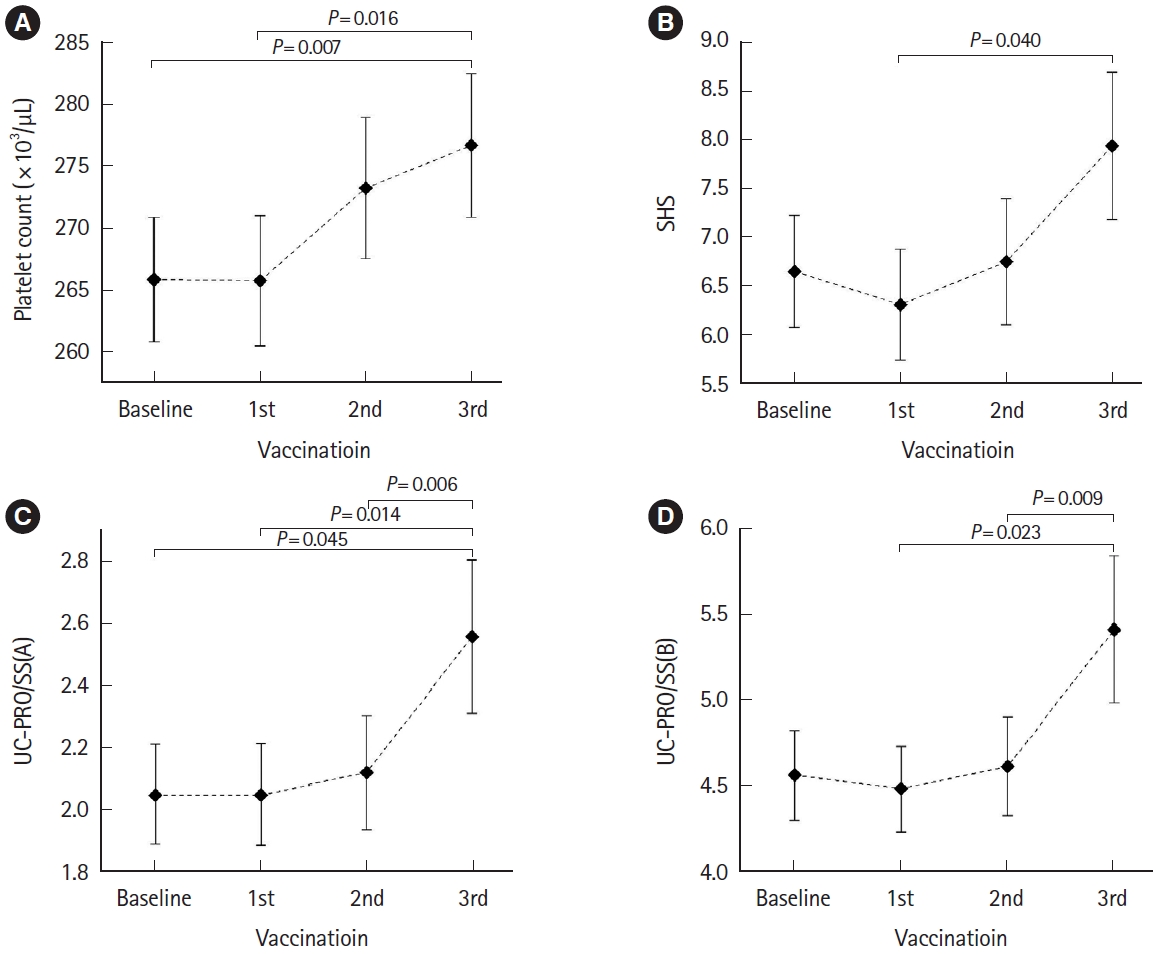
4. Comparison of Serial Variables According to Vaccination Orders
We compared the serial PRO scores and laboratory data obtained at baseline and after each vaccination using multiple pairwise comparisons (Table 7). In all patients, the platelet count significantly increased with continued vaccination. In patients with UC, SHS, UC-PRO/SS(A), and UC-PRO/SS(B) were significantly aggravated with continued vaccination. Moreover, there was no significant increase in the number of CD patients. The variables that significantly increased as vaccination continued are plotted in Fig. 2.
DISCUSSION
Concerns regarding adverse events after vaccination were a key factor behind the reluctance of patients with chronic immune-mediated diseases to be vaccinated against COVID-19 [19]. In this study, the incidence of adverse events after COVID-19 vaccination in patients with IBD was similar to that of a previous study with IBD patients and comparable to studies on the general population [20-22].
Several clinical studies have evaluated IBD exacerbation after vaccination against various viral and bacterial pathogens. In one prospective observational study, among 67 IBD patients vaccinated with the recombinant herpes zoster vaccine, only 1 (1.5%) experienced an IBD flare after vaccination [4]. In another prospective observational study, disease exacerbation related to the influenza vaccine was reported in 2 patients (2.2%) out of 92 with CD receiving anti-TNF [5]. According to one study assessing the change in IBD activity after pneumococcal vaccination, 10 of 306 patients (3.3%; 7 patients with CD and 3 with UC) experienced an increase in IBD activity within the 2-month follow-up [6]. In one meta-analysis study, the pooled incidence was 2% (95% CI, 1%-4%) when analyzing 10 studies regarding the exacerbation of IBD patients after receiving influenza, pneumococcus, recombinant herpes zoster, and hepatitis B vaccines [23]. However, little is known about whether COVID-19 vaccinations exacerbate IBD.
In a recent large controlled retrospective study to determine whether the COVID-19 vaccination was associated with a flare of disease in patients with IBD, there were no substantive differences in disease outcomes between vaccinated and unvaccinated patients [24]. In this study, the baseline disease severity of patients with IBD was assessed based on laboratory variables such as C-reactive protein, erythrocyte sedimentation rate, platelets, hemoglobin, white blood count, and albumin.
The recent focus of IBD treatment has shifted to its prevention and management, targeting both clinical and endoscopic remission using a ŌĆ£treat-to-targetŌĆØ approach [25]. Along with clinical remission, endoscopic healing, and absence of disability, restoration of quality of life is considered the most important long-term achievable treatment target for patients with IBD.
Various PROs have been developed, validated, and utilized in studies related to patients with IBD [10]. In this study, UC-PRO/SS and CD-PRO/SS, which met the U.S. FDA PRO guidelines for the first time, were used to assess disease aggravation [12,13].
We found that UC is an independent risk factor for worsening PROs in patients with IBD. In addition, SHS, UC-PRO/SS(A), and UC-PRO/SS(B) were aggravated significantly with continued vaccination in patients with UC, whereas there were no variables that increased risk significantly in patients with CD. Although the exact cause is not known, it could be due to the difference in pathophysiology between UC and CD [26]. The pathogenesis of IBD, including UC and CD, originates from a specific immunoinflammatory pathway, and it is known that T cells are one of the most important immune-related cells in this process [26-28]. However, T-cell profiles are disparate in UC and CD. T helper (Th) 1- and Th17-mediated immune responses are major processes in the pathophysiology of CD [26]. In contrast, atypical Th2 responses, mediated by natural killer T cells, are the main pathogenesis of UC [27,28]. Therefore, it can be speculated that the difference in T cell types involved in the pathogenesis of the 2 diseases causes a difference in the aggravation of PROs after vaccination. Translational research to precisely elucidate the mechanism of the influence of COVID-19 vaccination on the aggravation of PRO for UC is needed in the future.
In this study, young age was investigated as an independent risk factor for aggravating PROs in patients with IBD and UC. Recent studies have revealed that immunoglobulin G antibody titers against the SARS-CoV-2 spike protein and frequencies of neutralizing antibody titers after vaccination against COVID-19 were significantly higher in younger participants [29]. Therefore, it might be assumed that the elevated immune response in young patients influenced the aggravation of PROs in patients with IBD.
Male gender was identified as an independent risk factor for worsening PROs in patients with CD who received the COVID-19 vaccines in this study. In Asia, a higher prevalence of CD has been reported in males [30], and there has been a report identifying males as the sole risk factor for the occurrence of complications in CD [31]. This suggests that in Asian IBD patients, autoimmune responses exacerbating CD activity might occur more prominently in males than females. Based on this, a cautious inference can be made that the immune response to COVID-19 vaccination might have a more significant impact on disease exacerbation in males compared to females. Molecular-level studies on gender-specific immune responses after COVID-19 vaccination in IBD patients should be conducted in the future.
Our study found that IBD patients with aggravated PROs after vaccination had significantly higher baseline platelet counts than those without; moreover, platelet counts increased significantly with continued vaccination. Several recent studies have reported that platelet abnormalities and increased platelet counts are observed in patients with IBD, suggesting that platelet activation is an important factor in the pathogenesis and severity of IBD [32,33]. Increased platelet counts have also been considered as biomarkers for assessing disease activity in IBD [34,35]. Therefore, the findings related to platelets in this study are in line with those of previous studies.
To the best of our knowledge, this is the first study to evaluate the risk factors for aggravating PROs after COVID-19 vaccination in patients with IBD. In this study, as the patientsŌĆÖ PROs were investigated using a questionnaire survey, it was possible to comprehend the degree of disease exacerbation that the patients actually felt after vaccination. Moreover, ŌĆśclinically inactiveŌĆÖ patients who did not complain of apparent symptoms and had not changed their medication, including the dose for IBD treatment, within 1 year before the first vaccination were included in this study. This strict inclusion criterion enabled accurate detection of the vaccine effect in patients with IBD. Third, a well-controlled group of patients in terms of vaccination was included in the study to minimize selection bias. The rate of one or more doses of COVID-19 vaccination in Korea was 87.2%, and the rate of 2 or more vaccinations was 86.4% [36], which was much higher than the global rates of 63.9% and 29.2%, and the U.S. rates of 67.8% and 33.5% [1]. In addition, as patients were treated at 4 specialized IBD clinics in three large cities in Korea, patients were selected regionally without being concentrated in one region.
This study had several limitations. First, as the questionnaire survey was conducted during outpatient clinic visits, the results might have been influenced by recall bias. Second, the study enrolled 309 patients, a relatively small sample size. However, by including only patients defined as ŌĆ£clinically inactiveŌĆØ at the baseline through strict inclusion criteria, more accurate results were obtained despite the small sample. Third, due to limitations in sample size, patients who received all 5 types of COVID-19 vaccines were collectively analyzed. Future research should recruit more patients to assess the impact of each vaccine on IBDs. Fourth, the study did not investigate the types of medications taken by patients, suggesting a need for future research to explore if PROsŌĆÖ impact varies with medication type. Fifth, the study examined only baseline PROs before vaccination and PROs within 3 months after each vaccination, lacking data on whether the worsening of PROs persisted beyond the 3-month follow-up. Future research should examine disease exacerbation beyond 3 months post-vaccination. Sixth, information on patientsŌĆÖ endoscopic inflammation was not collected, indicating a need for subsequent research to determine if PRO changes correlate with endoscopic inflammation. Lastly, the study focused solely on South Korean participants and was conducted at 4 tertiary referral hospitals in different regions (Seodaemun-gu, Seoul; Songpa-gu, Seoul; Haeundae-gu, Busan; Jung-gu, Daejeon), with no significant differences in patient group characteristics among these hospitals. Future research should explore potential demographic, ethnic, or regional factors affecting study results.
In conclusion, PROs in patients with IBD, especially UC, worsened after vaccination against COVID-19, with the exception of patients with CD. Moreover, young age and UC were found to be independent risk factors for aggravating PRO. Therefore, there may be a need to counsel patients with IBD younger than 40 years of age and patients with UC before they receive COVID-19 vaccinations.