INTRODUCTION
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) characterized by relapsing and remitting mucosal inflammation which begins in the rectum with the potential to extend to proximal segments of the colon [1].
Clinical practice guidelines, including those from Japan, recommend oral corticosteroids (OCS) for remission induction in patients with moderate-to-severe UC; however, concerns against long-term OCS use given their adverse event profile and lack of evidence for maintenance of remission [2-4]. Japanese UC treatment guidelines recommend relatively high-dose OCS (30-40 mg, prednisolone equivalent) as an initial dose to determine its effectiveness then tapering and withdrawal within 3 months, followed by advanced therapy for OCS refractory or dependent patients [5]. In Japan, OCS prescribing for UC has generally fallen in line with increased use of thiopurines and biologics, and the proportion of patients with an OCS starting dose Ōēź 30 mg/day increased from 2011 to 2016 according to the previous findings from a retrospective claims database study [6]. However, many patients with UC still started OCS at lower doses, possibly due to physiciansŌĆÖ concern about adverse effects such as pneumonia and continued to use lower doses of OCS for extended periods of time. It was also found that long-term OCS use was most closely associated with low initial OCS dose ( < 10 mg/day) [6]. Another retrospective claims database study of Japanese patients with UC showed that OCS cycles were reinitiated and repeated several times even after OCS were discontinued, and up to 6 treatment lines were required before 10% of patients were administered biologics as a treatment option [7]. Significant number of patients with refractory UC in Japan may have not switched to advanced therapy due to prolonged OCS use.
A previous study utilizing an administrative claims database in the United States demonstrated the increased risk of pneumonia in patients with IBD, particularly those treated with corticosteroids (CS) [8]. With respect to Pneumocystis jirovecii pneumonia (PJP), a retrospective case-control study of Japanese patients with UC found that use of 3 immunosuppressive drugs, including OCS, was significantly associated with PJP with advanced age and lower lymphocyte count also noted as risk factors [9]. However, there is scant evidence as to whether the risk of pneumonia depends on initial OCS doses in patients with UC.
Based on this background, the primary objectives of this study were to assess: (1) the distribution of the initial OCS prescription dose in UC patients; (2) the prescription status of OCS; and (3) the incidence of pneumonia in each initial OCS dose treatment group. The secondary objective was to evaluate risk factors among UC patients who develop pneumonia, regardless of initial OCS dose. The exploratory objective was to describe other adverse events during the follow-up period by initial OCS dose treatment group.
In this study, a retrospective cohort of data from the Japan Medical Data Center (JMDC) claims database (JMDC, Inc., Tokyo, Japan) was employed to assess whether the incidence of pneumonia is increased with the guideline-recommended initial OCS doses.
METHODS
1. Study Settings
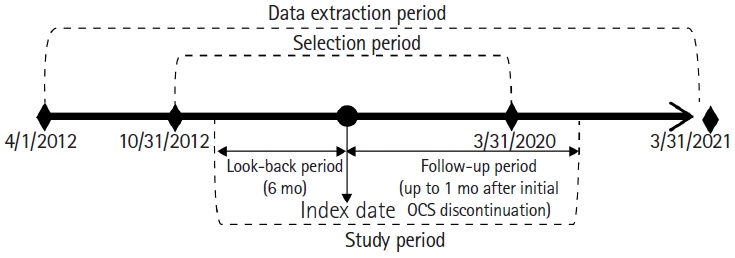
This claims database study employed the JMDC claim database and a propensity score (PS) matching method to control for related confounding variables. The data extraction period was from April 1, 2012 to March 31, 2021, with the selection period from October 31, 2012 to March 31, 2020 (Fig. 1). The index date was defined as the first OCS prescription after the UC diagnosis during the selection period while the look-back period was defined as the period of 6 months before the index date to examine the medical history and comorbidities and to assess the initial dose of OCS during the selection period. The follow-up period was set as the period after the index date to follow treatment status in UC and the occurrence of pneumonia. Patients were followed up until occurrence of any of the following events: occurrence of pneumonia, death, disenrollment from the JMDC claim database, end of data extraction period, and one month after the discontinuation of OCS. If there were no OCS prescriptions for more than 3 months from the end date of the OCS prescription, OCS prescribing was judged as being in a state of discontinuation.
The target exposure group was patients who received an initial OCS dose of 30-40 mg, as recommended by the treatment guidelines. The comparator treatment groups were those who received an initial OCS dose of either < 30 mg (lower initial OCS dose treatment group) or > 40 mg (higher initial OCS dose treatment group). Conversion of each OCS to prednisolone dose was calculated based on a dose equivalent conversion table [10].
2. Data Source
Data was sourced from the JMDC claim database, a commercially available, nation-wide insurer-based database from the Japanese health insurance system that contains both medical and pharmacy claims for approximately 14 million people insured by private health insurance and their dependents [11]. The JMDC database includes all claims data across any type of health facility, which captures the patient journey using a unique patient ID [11]. The JMDC database was selected because it: (1) mainly includes the working-age population, which represents the main cohort of patients with new onset of UC [12]; (2) collects claims not only from large facilities but also from clinics where may be the main health facilities to treat UC in Japan; (3) enables to provide relatively longer follow-up periods than other sources. Elderly-onset UC is recently on the rise in several countries, including Japan [13,14]. However, since they may also have lifestyle-related diseases such as diabetes, heart diseases, chronic lung disease, and cerebrovascular disease, etc. [15], which complicates assessment, this study focused more on patients with UC in the working-age population.
3. Inclusion and Exclusion Criteria
Patients aged Ōēź 15 years, had medical claims carrying an International Classification of Disease, Tenth Revision (ICD-10) code for confirmed UC (K51), received a colonoscopy assessment or UC drug (5-aminosalicylic acid products) prescription at the index date or within the look-back period, and initial OCS prescription at the index date were included. Patients exposed to initial OCS with prevalent UC were also included. Patients were excluded if they had medical claims of CrohnŌĆÖs disease (K50) at the index date or during the look-back period, or patients with medical claims of any pneumonia at the index date or during the look-back period. All diseases and drugs definition codes referred in this study were listed in Supplementary Table 1.
4. Outcomes
The primary outcomes were: (1) the distribution of the initial OCS prescription dose in UC patients, and (2) the incidence of pneumonia in each OCS dose treatment group. Pneumonia was defined as: (1) ICD-based diagnosis of pneumonia, and (2) prescription of antibiotics after use of OCS. PJP was defined as: (1) a diagnosis of PJP, and (2) a prescription of therapeutic doses (8 or more tablets) of trimethoprim-sulfamethoxazole (TMP-SMX) after OCS use. The prophylactic dose of TMP-SMX was defined as a prescription of 3 or fewer tablets per day. For descriptive analysis, the outcomes of interest were (1) distribution of patients receiving initial OCS dose ( < 30 mg, 30-40 mg, > 40 mg) at the index date; (2) total OCS doses, total prescription days of OCS, total visit count and hospitalization by the end of the follow-up period; (3) incidence of the first event of any pneumonia and PJP during the follow-up period; (4) patient background with or without prophylactic TMP-SMX prescription (3 or less tablets) at the index date; (5) adverse events other than pneumonia. For comparative analysis and risk factor analysis, the outcomes of interest were pneumonia by the end of the follow-up period. For descriptive and comparative analyses, all pneumonia events by the end of the follow-up period, including the index date, were counted as the outcome considering the risk of missing the occurrence of pneumonia due to OCS.
5. Study Sample Size
Based on the results of our feasibility analysis in advance, at least 700 patients were determined as sufficient patients to be collected for guideline-recommended initial OCS dose treatment group after 2:2:1 PS matching. The incidence of pneumonia was estimated to be 1.5 or 2 times higher in the high-risk group than in the low-risk group. We assumed the incidence rate of pneumonia as 7.5% in the high-risk group and 5.0% in the low-risk group with an estimated relative risk of 1.5 (95% confidence interval [CI], 1.00-2.29) and the incidence rate of pneumonia as 10.0% in the high-risk group and 5.0% in the low-risk group with an estimated relative risk as 2.0 (95% CI, 1.35-2.96).
6. Statistical Analysis
Generalized PS matching was employed to compare the baseline characteristics between each OCS dose treatment group for minimizing the effect derived from confounding factors. Generalized PSs were calculated by multinomial logistic regression. Standardized mean difference (SMD) was calculated before and after matching to identify differences in patient background factors between OCS treatment groups. A ratio of 2:2:1 caliper width matching was performed using generalized PSs. IR, incidence rate ratio (IRR), and 95% CI were calculated in the matched population based on the person-year method. Adjusted IRR, using covariate factors of matching, was calculated by Poisson regression. Risk factor analysis was performed with Poisson regression in the population before matching with potential risk factors considered in the model including age, sex, bed numbers at the index date, comorbid allergic disease (allergic rhinitis, asthma, atopic dermatitis), and the Charlson Comorbidity Index (CCI) during the look-back period. CCI on receipt data followed QuanŌĆÖs method [16]. Data extraction from the database was performed using Amazon Redshift and SQL (Amazon Web Service Inc., Seattle, WA, USA). All other analyses were conducted using R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
1. Patient and Treatment Characteristics
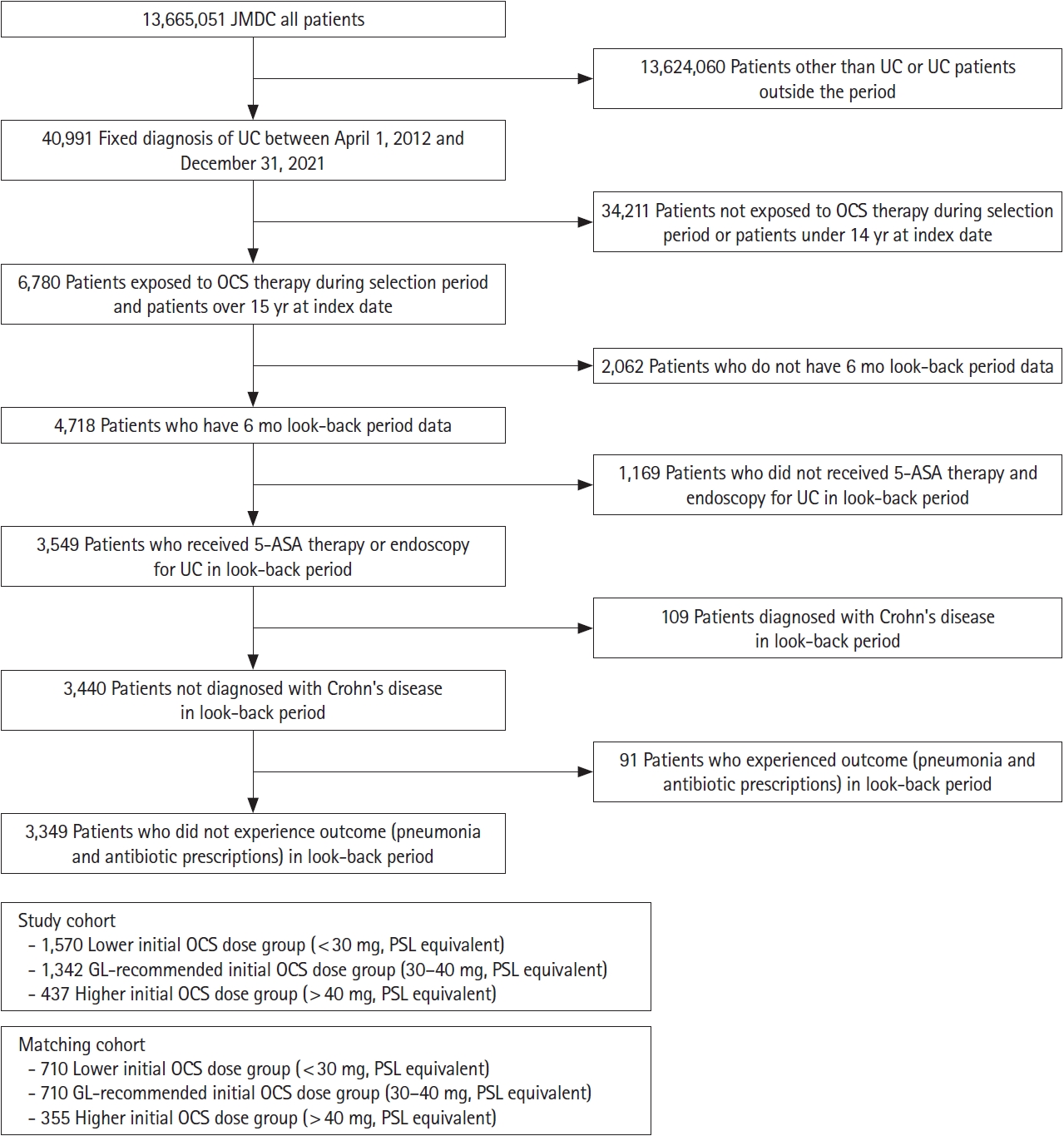
All patients enrolled in the JMDC claim database (n = 13,655,051) were considered and screened according to the eligibility criteria (Fig. 2). After screening, a total of 3,349 patients comprised the whole cohort ( < 30 mg, n = 1,570; 30-40 mg, n = 1,342; > 40 mg, n = 437) and 1,775 patients comprised the matched cohort using a generalized propensity matching score in a 2:2:1 ratio ( < 30 mg, n = 710; 30-40 mg, n = 710; > 40 mg, n = 355) (Fig. 2). Patient characteristics at the index date and during the 6-month look-back period before and after PS matching are shown in Table 1. By PS matching, SMD was reduced in the matched cohort compared with the unmatched cohort.
2. OCS Treatment
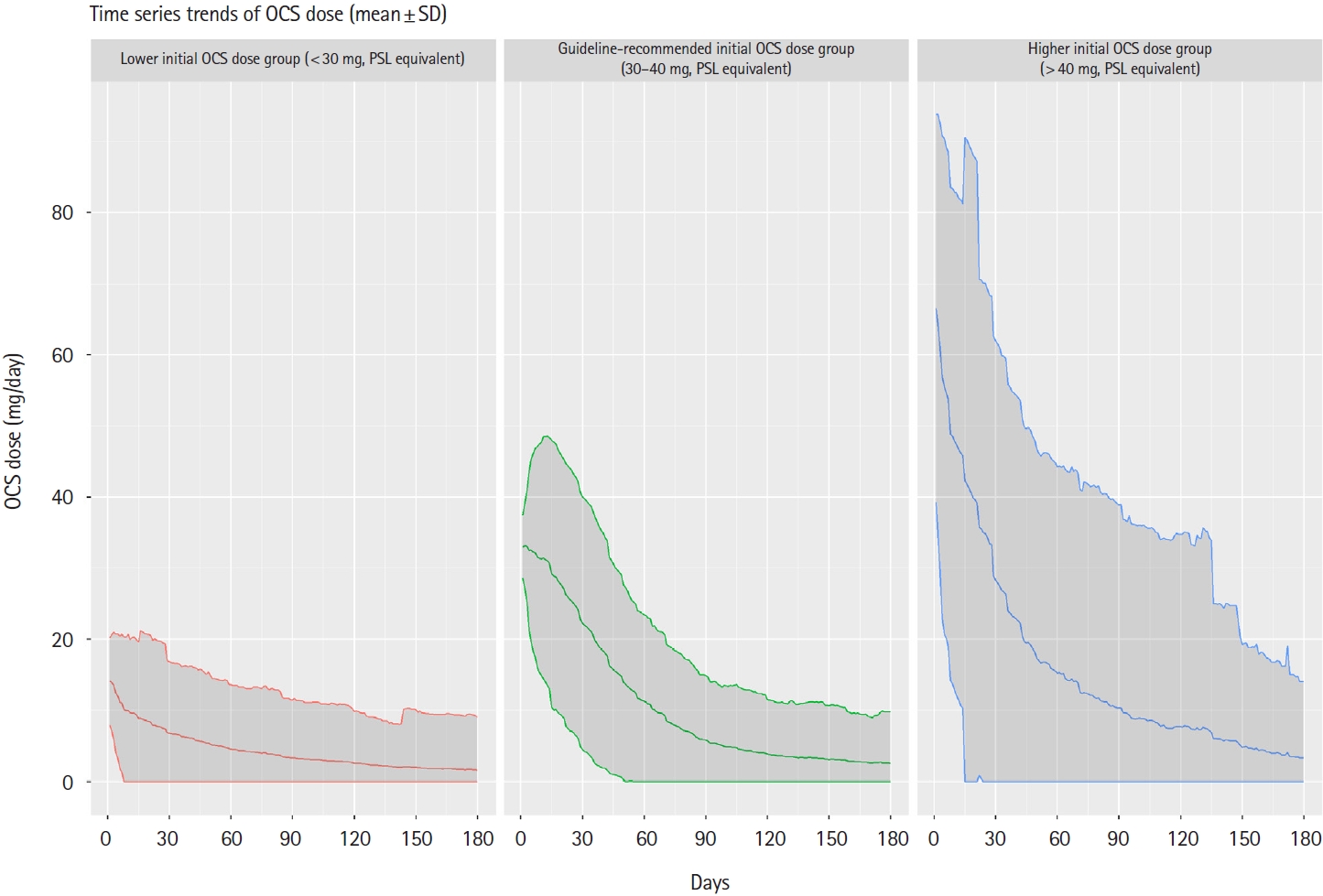
The distribution of patients in the whole cohort prior to matching showed that nearly half of the patients used lower doses than those of guideline recommendations (Table 1). The distribution of the initial OCS prescription dose according to the matched cohort is summarized in Table 2. The median total duration of OCS treatment was 45.5 to 78.5 days across the initial dose subgroups. The mean total duration of OCS treatment was greater than the median total duration of OCS treatment across treatment groups, and the maximum total duration of OCS treatment was greater than 2,000 days across treatment groups (Table 2). The lower initial OCS dose treatment group was further subdivided into < 10 mg, 10 to < 20 mg, and 20 to < 30 mg as detailed in Supplementary Table 2. The proportions of patients who received OCS for longer than 180 days were nearly 20% or less across subgroups. Furthermore, we found that regardless of the initial dose, OCS were tapered and discontinued within 180 days in most patients (Fig. 3). The mean total visit count was approximately 6 across OCS treatment groups (Table 2). There was no difference in hospitalization rates across OCS treatment groups throughout the follow-up period (Table 2).
3. Incidence and Risk of Pneumonia
The IRs of any pneumonia in association with antibiotic treatment in each OCS dose group are detailed in Fig. 4. Overall, the incidence of any pneumonia with antibiotic prescription was low and the IRs of any pneumonia were similar across OCS treatment groups (Fig. 4). The adjusted IRRs, using covariate factors of matching, for the lower and higher initial OCS dose treatment groups compared with the guideline-recommended initial OCS dose treatment group were low; however, 95% CI for both crude and adjusted IRR straddled 1.0, thus the results did not show a difference between these treatment groups (Fig. 4). The diagnoses of all pneumonia events, identified by the ICD-10 codes, can be found in Supplementary Table 3. There were no PJP with therapeutic doses of TMP-SMX prescription found in the matched cohorts.
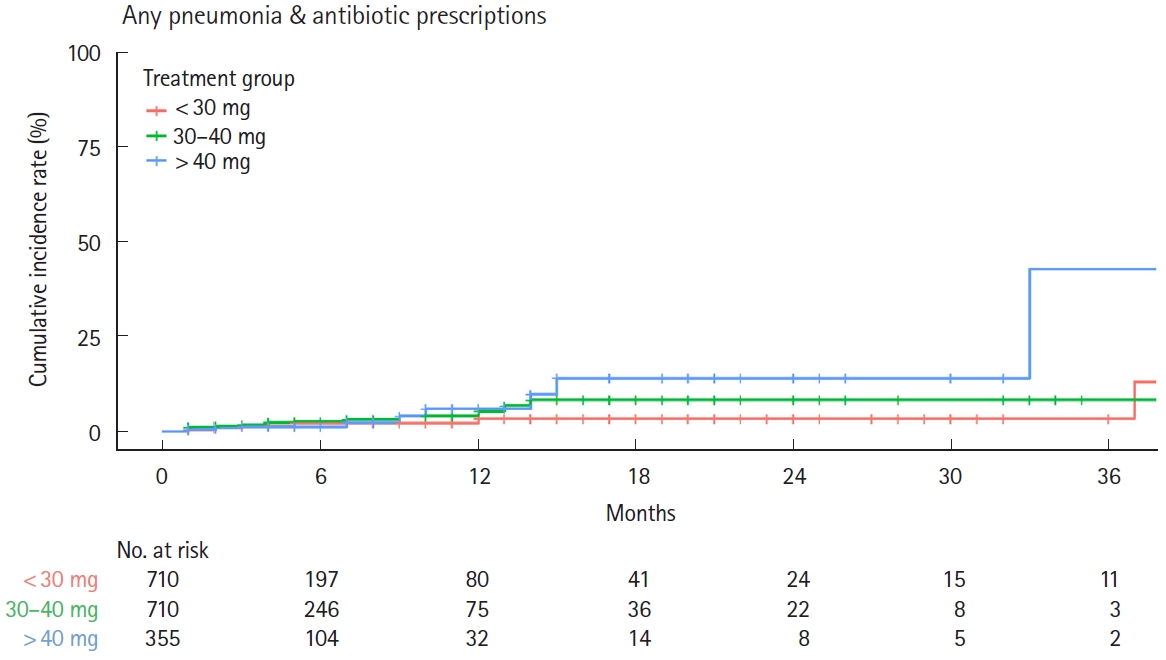
Time to any pneumonia events in each OCS treatment group is shown in Fig. 5. The cumulative incidence of pneumonia was low in all OCS treatment groups within 6 months of OCS administration and did not differ across OCS treatment groups; however, the incidence of pneumonia tended to increase after 12 months of continuous OCS administration (Fig. 5). As for prognosis of any pneumonia patients, no deaths occurred during the follow-up period.
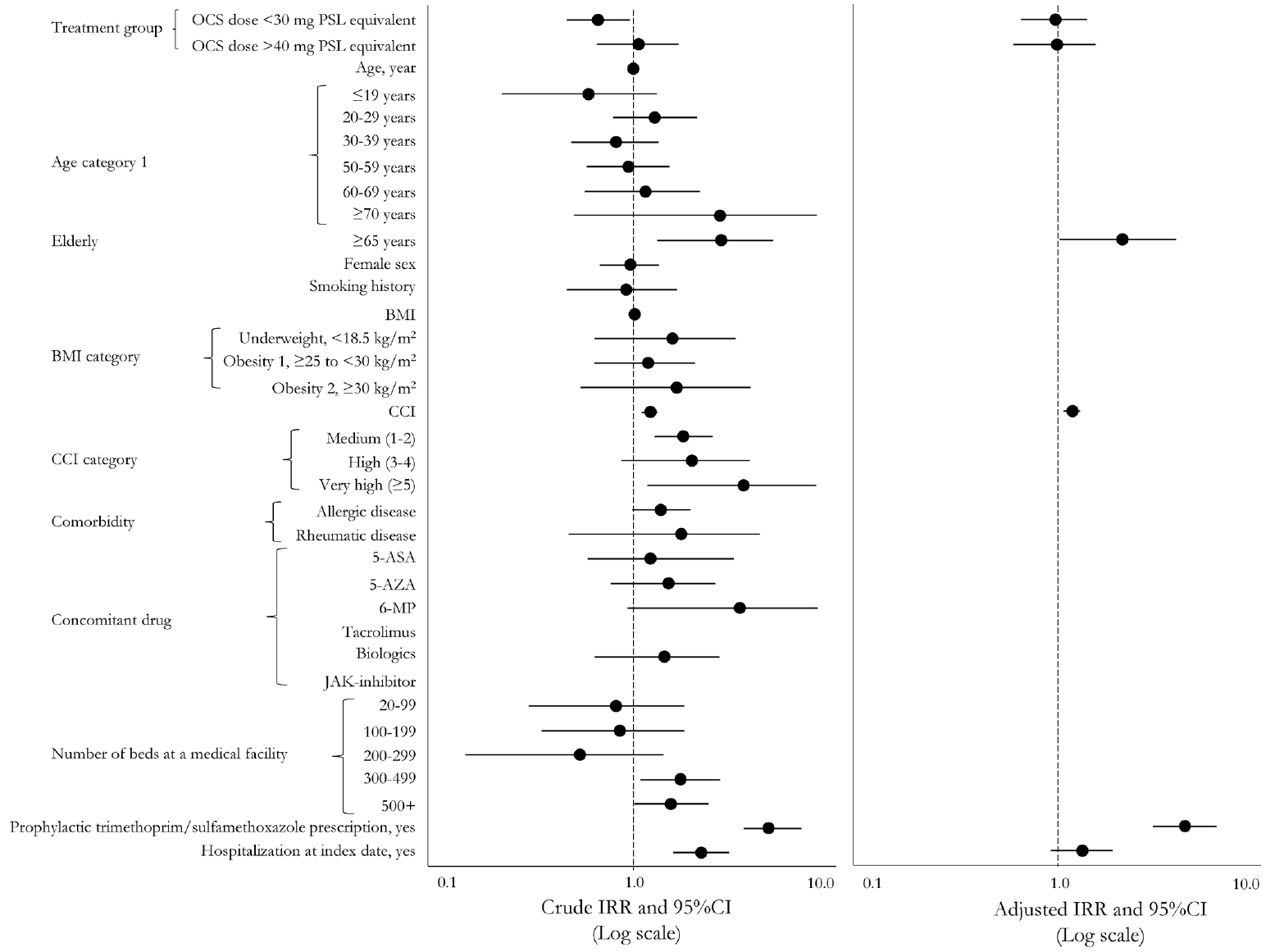
The IRRs of any pneumonia in the present study (before PS matching) cohort are shown in Fig. 6 and Table 3. Risk factors associated with any pneumonia were advanced age ( Ōēź 65 years), higher CCI score, in large facilities with bed numbers > 300 or > 500, prophylactic TMP-SMX treatment, and being hospitalization at index date (Table 3, Fig. 6). A total of only 3 cases of PJP (1 case in the lower initial OCS dose treatment group, 2 cases in the guideline-recommended initial OCS dose treatment group) were found in the whole cohort; patient backgrounds of these 3 PJP cases are shown in Table 4.
A positive correlation was found between prophylactic antibiotics and the development of pneumonia. Specifically, the adjusted IRR for patients with any pneumonia who received prophylactic TMP-SMX compared with patients who did not receive TMP-SMX was 4.87 (95% CI, 3.26-7.24), and the 95% CI exceeded 1.0 for both crude IRR and adjusted IRR. Patient background in the groups with and without prophylactic TMPSMX prescription showed that the patients receiving prophylactic TMP-SMX prescription had numerically higher age ( > 60 years), higher CCI index, higher concomitant immunosuppressants (azathioprine or biologics) use, in larger facilities with bed numbers > 300 or 500, and in more hospitalizations rate at an index date than the group without (Supplementary Table 4).
In terms of the exploratory endpoint, a wide range of other adverse events occurred during the follow-up period in each initial OCS dose treatment group as shown in Supplementary Table 5. Frequent events, occurring in more than 5% in any initial OCS dose treatment group, included common medical conditions such as acute bronchitis, acute pharyngitis, acute upper respiratory infections, acute nasopharyngitis, allergic rhinitis, dermatitis, asthma, acne, dorsalgia, conjunctivitis, disorders of refraction and accommodation, and medical conditions that are commonly complicated by UC such as hemorrhoids and perianal venous thrombosis, volume depletion, sleep disorders, and iron deficiency anemia. The incidence of these comorbidities did not differ across the OCS treatment groups. The incidence of gastric ulcer was high. This may be because a diagnosis of gastric ulcer was given to prescribe proton pump inhibitors for the prevention of gastric ulcer. The incidence of other adverse events was similar between initial OCS dose treatment groups with the main exceptions being a lower incidence of glaucoma and a higher incidence of polyneuropathies in the higher initial OCS dose treatment group. Adverse events such as type 2 diabetes and osteoporosis, for which long-term administration of OCS is considered a risk factor, were infrequent and did not differ across OCS treatment groups.
DISCUSSION
The present study demonstrated that the duration of OCS treatment in the lower initial OCS dose treatment group was shorter than in the guideline-recommended initial OCS dose treatment group. The proportion of long-term use exceeding 180 days was less than previously reported [6], regardless of the initial OCS dose. However, patients with excess dose and duration of OCS prescription were rare although still existed. The incidence of any pneumonia in UC patients receiving OCS was low and did not differ by the initial dose of OCS. The incidence of PJP was rare, and there was no clinically relevant difference in the initial dose of OCS. The onset of any pneumonia was less frequent within 180 days across OCS treatment groups. The risk factor of any pneumonia was identified as follows: age > 65 years, higher comorbidity, treated in larger hospital with > 300 beds, and being hospitalized. Prophylactic TMP-SMX was found to be more frequently administered to patients with these risk factors.
Our study findings using a PS matching method focusing on Japanese UC patients provided important implications for clinicians. Firstly, the apparent risk of any pneumonia remained low regardless of the initial OCS dose. A previous report suggested that physicians may prefer to use lower initial doses of OCS to mitigate the development of adverse events such as pneumonia [6], and the present study also found that the proportion of patients starting at low doses of OCS remained high. Key differences between previous and the present retrospective database claims study are noteworthy. A previous report used the same JMDC claim database covering the data from 2006 to 2016, when the initial OCS doses of < 10 mg may have significantly associated with long-term use of OCS [6]. Additionally, nearly half of patients were prescribed long-term OCS for more than 180 days since 2014 [6]. In contrast, 60% of patients in the present study who started OCS < 10 mg had a shorter dosing period of < 30 days and fewer patients used OCS for > 180 days. Recently, a single-center study by Masuda et al. [17] also reported a decrease in the duration of OCS use over the last 10 years. Therefore, treatment trends may have changed in recent decades, possibly in response to the greater penetration of advanced therapies including biologics [18-23] and a better awareness of the proper use of OCS for exacerbations.
Secondly, the risk of PJP was extremely low in patients who received any dose of OCS. There were no PJP cases found in the matched cohort, and a total of 3 PJP cases found from the whole cohort before PS matching. The present study was consistent with the previous report of 4,525 Japanese UC patients, showing no cases of PJP after 2014, when the prophylactic TMP-SMX was prescribed to high-risk patients [9]. These findings support the use of guideline-recommended initial dose of OCS; the use of prophylactic treatment could be considered based on risk factors rather than reduced starting dose of OCS. To follow the treatment steps according to the treatment guidelines, it is desirable to start with a sufficient dose of OCS (30-40 mg) and to determine the effectiveness of OCS at an early stage.
Across the pneumonia types, several background risk factors seemed to be consistently present in the whole cohort regardless of initial OCS dose, including elderly ( > 65 years old), elevated CCI score, various concomitant UC therapies, treated in larger medical facility > 300 beds, and hospitalization at an index date. Previous research has suggested that obvious risk factor for PJP include advanced age, low lymphocyte counts during treatment with immunosuppressive drugs, and use of 3 or more immunosuppressants in Japanese patients with UC [9]. In our study, the IRR for pneumonia was numerically higher in patients prescribed 3 or more concomitant medications including OCS, although this difference was not statistically significant (Table 3). The present study provided additional findings on risk factors to consider. Patients with multiple comorbidities, visiting larger facilities and being hospitalized at an index date, showed a higher risk for pneumonia. Hospitals with larger bed capacity are often tertiary centers, potentially treating severe UC patients or elderly patients with comorbidities. These patients may have an increased risk of developing pneumonia. Consequently, this might explain the increased risk of pneumonia in medical facilities with 300-499 or Ōēź500 beds. This might indicate that care for comorbidities need to be considered especially for elderly individuals and severe UC to reduce the risk of pneumonia [24]. Prescription of prophylactic TMP-SMX during the use of OCS was found to be common in patients at high-risk, although only 41 patients had prophylactic prescription among UC patients (Supplementary Table 4). Since patients who developed pneumonia were given prophylactic TMP-SMX at the physicianŌĆÖs decision, this may imply that prophylactic TMP-SMX prescriptions are an identifiable risk factor for pneumonia.
In this study, we observed that the incidence of pneumonia within 6 months following OCS administration was constantly low across all initial OCS dose groups. Moreover, the proportion of patients who had been on OCS for more than 180 days was 20% or less (Table 2). As a result, the incidence rate of pneumonia remained low in this study. These findings underscore the importance of evaluating the effectiveness of OCS within the first 4 weeks or reducing below the equivalent of prednisolone 10 mg/day within 3 months, in line with the recommendations of the European CrohnŌĆÖs and Colitis Organization and switching to thiopurines or advanced therapy when a patient exhibits OCS refractory or dependency to mitigate the risk of adverse events [25,26].
The treatment guidelines also recommend tapering OCS to 10 mg or less within 3 months [5]. In this study, we found that, regardless of the initial dose, OCS were tapered and discontinued within 180 days in most patients (Fig. 3). This suggests that recent practice may be in alignment with guideline recommendations.
Higher doses of CS are usually administered intravenously compared to oral administration. As such, patients receiving intravenous CS may be the population most at risk for pneumonia and could be used as a high-dose group. However, according to the Japanese treatment guidelines for UC [5], high-dose intravenous CS are recommended for patients who do not respond to OCS or suffer from acute severe UC, and the effectiveness of intravenous CS should be evaluated within 1-2 weeks to determine whether colectomy is indicated or switch to advanced therapy [27]. Given the different usage of intravenous CS compared to OCS, we did not classify patients who initially received intravenous CS as the high-dose group.
Although PJP is rare in the general population, the incidence of PJP is higher in IBD patients and PJP is reported to be highly lethal once it occurs [8,28,29]. Advanced age, lower lymphocyte counts and use of multiple immunosuppressants, such as OCS, thiopurine, and anti-tumor necrosis factor therapy have been reported as risk factors for PJP [9,30], and prophylactic prescribing of antibiotics using TMP-SMX has been recommended for the prevention of PJP [9,31]. Another study showed that routine administration of PJP prophylaxis in IBD patients treated with OCS, immunosuppressants, and biologics may not be warranted, since there were low risks of PJP despite the uncommon use of prophylactic antibiotics [32]. In this study, a total of 3 PJP cases were detected in the whole cohort before PS matching, and it was found that prophylactic TMP-SMX was not prescribed for 2 out of these 3 patients. Although it could not be determined whether prophylactic administration of antibiotics was necessary to prevent PJP and pneumonia, these results showed that prophylactic TMP-SMX were prescribed commonly to patients at high risk, and clinical significance of this study is that it could provide evidence that the incidence of pneumonia including PJP were low regardless of the initial dose if OCS was used within 6 months.
The incidence of other adverse events such as type 2 diabetes, peptic ulcer and osteoporosis, which are considered as typical adverse events of long-term administration of OCS [33] occurred less frequently and showed no notable difference across OCS dose treatment groups during the follow-up period. However, this may not have been evaluated due to the limitations of the JMDC claim database, which has limited data on the elderly, and may need to be evaluated using a different data source if necessary.
The main strength of this study is that this research reflected the treatment environment in recent decades and evaluated the risk of pneumonia and PJP in more than 3,000 Japanese UC patients, focusing only on patients receiving OCS. The use of the JMDC database, which contains both medical and pharmacy claims representing approximately 14 million people insured by private health insurance [11]. Specifically, JMDC provided several advantages in that the onset of UC is most frequent in the working-age population [12] and UC maintenance treatment and prescriptions are mostly given in clinics. Therefore, it seems reasonable to use a traceable medical database.
The main limitation of this study is that the definitions of pneumonia and PJP were not validated. Smoking history and body mass index, which may affect pneumonia, were not considered in the matching factors and multivariate analysis due to missing values of only limited to patients receiving health examinations. Body weight and body surface area, which may be used as the basis for initial OCS dosing were not available in the JMDC database. As for vaccination, the European consensus statements on the prevention, detection, and management of opportunistic infections in IBD indicate the importance of vaccination for high-risk patients [31]. However, vaccination records for pneumonia are not available in the JMDC database because it comprises healthcare insurance claims, and vaccinations are not covered by Japanese healthcare insurance. The disease status of UC and clinical test results are not available. The possibility of misclassification of CrohnŌĆÖs disease exists when the ICD code only is used as an exclusion criteria. Further, it is not possible to specify the purpose of OCS and antibiotic prescription, which may confound the results. Finally, access to data for elderly people was insufficient in the JMDC database because data were derived from healthcare insurance for working people.
In conclusion, the results of this Japanese claim database study demonstrated that the proportion of patients starting at low OCS dose ( < 30 mg) remained high. The percentage of patients using OCS for longer than 6 months was lower than previously reported. The incidence of pneumonia, including PJP, among Japanese UC patients was extremely low across initial OCS dose treatment groups. Patients with multiple risk factors may require, for example, care for lifestyle-related diseases and avoidance of long-term use of OCS. Following the guideline-recommended initial OCS dose may allow rapid determination of its effectiveness and benefit patients with UC by switching to advanced therapy earlier.