INTRODUCTION
Coffee is one of the most widely consumed beverages worldwide and is a major source of dietary antioxidants [1]. Several groups have previously reported that coffee or caffeine (1,3,7-trimethyxanthine, also abbreviated to CAF) consumption reduces both the frequency of liver disease [2,3] and the incidence of cancer [4,5]; these effects appear to be mediated by inhibition of cell proliferation [6,7] and enhancement of autophagy via PI3K (phosphatidylinositol-3 kinase)/Akt (protein kinase B)/mTOR inhibition [8]. Some reports strongly suggest the anti-inflammatory and antioxidant effects of coffee extracts and selected constituents (including CAF and kahweol) in intestinal inflammation [9-13]. Although the anti-inflammatory and anti-tumor effects of CAF have been reported by many groups in several organs, the possibility for coffee (but not only CAF) to affect intestinal inflammatory diseases is still controversial, as nicely reviewed by 2 recent review articles [14,15]. Notably, coffee is likely to play a protective role in mucosal inflammation based on a meta-analysis of the association between Crohnâs disease (CD) and beverage intake [16]. However, the biological mechanisms underlying the CAF-mediated effects on colonic epithelial cells (CECs) and colon cancer, especially colitis-associated cancer, remain controversial for almost the past 2 decades [17-21] and have not been fully explained scientifically.
As one of the CAF-oriented research groups, we do not intend to discuss the detail of immunological or biological mechanisms of action on low-dose CAF and sugar (mainly sucrose) combinational administration in the incidence of inflammation-associated carcinogenesis, but we would like to suggest new possibilities for the relationship between the 2 factors in a chronic colitis model, of which may throw a stone into the controversy over the effects of CAF under intestinal inflammatory conditions in this review.
CAF BELONGS TO THE GROUP OF METHYLXANTHINE DERIVATIVES, WHICH ARE KNOWN AS PAN-CHITINASE INHIBITORS
CAF belongs to a group of alkaloid chemicals, so-called methylxanthines, which originated from purine-based xanthine [22]. Methylxanthines, as the name suggests, are methylated derivatives and include compounds such as CAF, theophylline, pentoxifylline (PTXN), aminophylline, theobromine, paraxanthine, 3-isobutyl-methylxanthine, and so on. Several methylxanthine derivatives are known as chitinase inhibitors [23]. SchĂźttelkopf et al. [24] have demonstrated clearly that 2 linked CAF moieties specifically bind in the active site of pan-family 18 chitinases (which family includes most of the mammalian and bacterial chitinases) and work as the inhibitor of these enzymes, as shown by X-ray crystallography. Interestingly, methylxanthine derivatives, including CAF, PTXN and theophylline, and the family 18 chitinases show a similar form of binding and have a common position for docking revealed by X-ray diffraction analysis [23].
If compared with a parameter of IC50 (half maximal inhibitory concentration), PTXN (126 Îźmol/L) shows 4 times and 12 times higher chitinase inhibitory effect as compared to CAF (469 Îźmol/L) and theophylline (1,500 Îźmol/L), respectively [23]. However, the above 3 methylxanthine derivatives show a significantly lower affinity against fungal chitinase than allosamidin (IC50: 10 Îźmol/L), a chitinase derived from Candida albicans [23]. Within the mammalian chitinases, enzymatic inactive chitinase 3-like 1 (CHI3L1, also known as YKL-40) has been identified as a critical factor in regulating the innate and acquired immune responses in chronic inflammatory diseases including asthma, chronic obstructive pulmonary disease, and inflammatory bowel disease (IBD) [25-28]. For these reasons, methylxanthine derivatives have the potential to be useful as chitinase inhibitors, including CHI3L1 and acidic mammalian chitinase, in chronic inflammatory disorders as well as inflammation-associated cancers [25,29].
COMMONLY ACCEPTED CONCEPTS AND ACTUAL EXAMPLES ABOUT THE COFFEE/CAF INTAKE IN GENERAL
CAF is the most widely recognized psychoactive compound in the world and is found in a wide variety of beverages and foods, which are consumed by men, women, and children of all ages [30,31]. CAF is also easily absorbed through the digestive tract [32], and the U.S. Food and Drug Administration recommends that CAF has no dangerous adverse effects on health if consumed in amounts up to 400 mg per day (4-5 cups of coffee).
The structural similarity of CAF to adenosine causes it to bind to the adenosine A2A receptor, resulting in the induction of an antagonistic effect of CAF on adenosine, which promotes arousal and insomnia [33-35]. Additionally, CAF has also been postulated to be involved in a wide range of physiological activities, including nonselective inhibition of phosphodiesterase [36], sensitization of calcium channels [37], antagonism of Îł-aminobutyric acid receptors,38 stimulation of adrenal corticosteroids [39,40], and improvement of glucose metabolism by enhancing insulin responsiveness through inhibition of glucose absorption [41]. Moderate consumption of CAF (coffee) is thought to have beneficial associations with pain, reduced risk of type 2 diabetes [42,43], Parkinson and Alzheimer disease [44], and reduced risk of developing colon cancer [45], kidney as well as liver diseases (Fig. 1) [46]. In contrast, the consumption of CAF-rich products has potential risks such as anxiety, insomnia, tremors, and palpitations (Fig. 1).
Bessler et al. [9] have shown that coffee consumption may generally reduce the inflammatory process in the colon and lower the risk of colorectal cancer (CRC) mortality for several mechanistic reasons. In addition, large amounts of coffee consumption (4-6 cups or more per day) have been suggested to reduce the risk of developing colitis-associated cancers [45]. Furthermore, caffeinated coffee consumption has been suggested to reduce the overall risk of CRC [20] and may be associated with reduced recurrence and death in patients with stage III CRC [47]. However, a similarly low incidence of CRC has been observed with a higher intake of decaffeinated coffee [20,48]. Moreover, some studies have reported no useful data to support an association between CAF intake and the risk of developing CRC [49]. Therefore, the association between CAF intake and CRC incidence is still controversial. We have summarized the overall pros and cons of coffee/CAF intake in colonic inflammation and CRC later in this review article.
Moderate coffee intake has been suggested to have beneficial effects (hepatoprotective effect) on various liver diseases, including alcoholic liver disease [50], nonalcoholic fatty liver disease [51,52], liver cirrhosis [53], hepatitis caused by hepatitis B virus [54], and hepatitis C virus [55], possibly by inhibiting the binding of adenosine to its receptor [56,57]. Furthermore, espresso coffee has been shown to have no beneficial effect on liver disease, particularly nonalcoholic fatty liver disease [58]. This may be due to the effect of the addition of sucrose, which is composed of glucose and fructose, to the coffee, which may counteract the effect. Fructose has also been associated with increased severity of liver fibrosis in nonalcoholic steatohepatitis [59]. Thus, the hepatoprotective effect of coffee may depend on various factors, such as the presence or absence of additives (sucrose, etc.), and the impact of these factors should be studied in the future.
ORAL CAF ADMINISTRATION AMELIORATES INTESTINAL INFLAMMATION IN A MOUSE ACUTE DSS-INDUCED COLITIS MODEL
Many studies reported that xanthine derivatives have anti-inflammatory effects. Paiva et al. [60] conducted a systematic review, showing that CAF intake upregulates interleukin (IL)-10 on serum levels. Freedman et al. [61] performed the most extensive cohort study (229,119 men and 173,141 women over 14 years) in 2012 and revealed a dose-dependent inverse association between coffee drinking and total mortality. The primary anti-inflammatory mechanisms result from the nonselective inhibition of phosphodiesterase and the nonselective antagonist of the adenosine receptor. These effects cause the activation of protein kinase A, leading to the inhibition of pro-inflammatory cytokine production, such as tumor necrosis factor Îą (TNF-Îą). Nevertheless, some studies insist that CAF consumption induced limited anti-inflammatory effects [62]. Here we reviewed some possible mechanisms of the anti-inflammatory effects of xanthine derivatives on IBD utilizing a colitis mouse model.
IBD is well-known as a group of intestinal inflammatory disorders, which includes CD and ulcerative colitis (UC). Our group previously reported that CECs and macrophages produce CHI3L1 during acute and chronic phases of colitis in the murine colitis models [63]. CHI3L1 in colonic tissue samples of CD and UC patients is upregulated compared to inactive CD and UC patients, and normal individuals positively correlated to the severity of colitis [63]. CHI3L1 has been reported as a significant mediator in many inflammatory disorders, such as asthma, hepatitis, and rheumatoid arthritis [64-67].
It is well-known that dysregulated host-microbial interactions lead to the development of intestinal inflammation in IBD [68,69]. Therefore, possible pathogenic commensal bacteria invasion into CECs could relate to the pathogenesis of IBD. Our group previously revealed that CHI3L1 mediates PI3K/Akt signaling in CECs, enhancing the secretion of IL-8 and TNF-Îą in a concentration-dependent manner [70]. Several studies have shown that Akt signaling increases in colitis mouse models, CD, and UC patients [71,72]. Conversely, IBD patients on 5-aminosalicylic acid treatment exhibited reduced levels of active phosphorylated Akt in inflamed colitis tissue, suggesting a positive correlation between colitis severity and Akt signal activation [73]. Given these mechanisms, CHI3L1 could play a significant role in colitis in IBD. Therefore, we hypothesized that xanthine derivatives, pan-chitinase inhibitors, could be a novel therapeutic strategy for IBD by suppressing the CHI3L1 expression and activation.
To explore how xanthine derivatives work on IBD, we first conducted in vitro experiments. We incubated SW480 (a human colon cancer cell line) with 2.5 mM or 5 mM of CAF. Subsequently, we treated them with adherent-invasive Escherichia coli (AIEC) as potential pathogenic bacteria in the normal flora. After gentamycin treatment to eliminate the extracellular AIECs, the SW480 were stained with anti-E. coli lipopolysaccharide antibody. The 2.5 mM CAF treatment group showed a reduced number of intracellular AIECs compared to the control group. Moreover, the 5 mM CAF treatment group showed fewer intracellular bacteria [74]. CHI3L1 mRNA expression in SW480 was also reduced in a dose-dependent manner by incubating with CAF [74]. This result suggested that CAF could prevent AIECs invasion into CECs by decreasing the expression of CHI3L1. Theophylline and PTXN showed reduced CHI3L1 mRNA expression in a dose-dependent manner as well [22].
Given these results, we shifted to in vivo experiments using C57BL/6J wild-type (WT) mice, which were purchased from The Jackson Laboratory (Bar Harbor, ME, USA), to examine the anti-inflammation effect of CAF in an acute colitis model. Those mice were first treated with CAF in their drinking water for 7 days, followed by 3.5% dextran sulfate sodium (DSS) with CAF for 5 days. Normal drinking water was given for an additional 7 days until the mice were sacrificed. The mice treated with CAF showed resistance to body weight loss and enhanced body weight and clinical score recovery after DSS treatment compared to the control group of mice [74]. Consistent with the in vitro experiment, mRNA expression of CHI3L1 was completely suppressed in the CAF-treated mice [74]. The colonic histology displayed milder colitis and less inflammatory cell infiltration in the CAF-treated mice compared to the control [74]. Inflammation-associated cytokines (TNF-Îą, IL-17F, interferon-Îł, and IL-4) were decreased, and anti-inflammatory IL-10 was increased in colons of the CAF-treated mice compared to the control [74]. In conclusion, we demonstrated that CAF ameliorates acute DSS-induced colitis by suppressing CHI3L1 expression and its functions.
Similarly, another animal model of colitis treated with other xanthine derivatives exhibited protective effects: Theophylline treatment reduced myeloperoxidase activity and TNF-ι, IL-1β, and IL-6 in the colons in an acetic acid-induced colitis rat model [75]. Karatay et al. [76] treated trinitrobenzene sulfonic acidinduced colitis rat model with PTXN intraperitoneal or intrarectal injection. Both groups displayed reduced damage in colitis by PTXN, but the intraperitoneal route was more effective.
Although many in vivo studies support the positive effect of the xanthine derivatives, there is no clear evidence between coffee consumption and human IBD flare. According to the in vivo studies, regular intake of a suitable amount of CAF may prevent intestinal inflammation, especially in IBD gene susceptible individuals. Barthel et al. [77] conducted a questionnaire among IBD patients in Switzerland. Seventy-two point six percent of the total 442 patients regularly drink coffee, and 91% of the group reported no impact of coffee consumption on IBD. Recently, Georgiou utilized Mendelian randomization analysis to evaluate the effect of the exposure factor, smoking, coffee, and alcohol, on CD and UC risk. They revealed that there is no clear evidence that either is related to the risk of CD or UC [78]. Compared to the xanthine derivatives, coffee is a mix of complex compounds; some might work with counteractive effects to the anti-inflammatory mechanisms. Moreover, before it reaches the intestine, coffee is absorbed throughout the digestive tract. Therefore, although CAF may have some effect in colitis mouse models, many factors could explain why coffee intake does not demonstrate apparent protective effects on human IBD.
PROS AND CONS OF COFFEE/CAF INTAKE ON THE EFFECT OF INFLAMMATION AND CARCINOGENESIS IN THE COLON
As summarized in Table 1, the effects of CAF intake on the effect of inflammation and carcinogenesis in the colon are highly controversial. Although coffee/CAF intake seems to reduce the inflammatory responses in the colon [9,74,79], recent 2 reports suggest that CAF consumption is positively associated with the prevalence of CD or UC [75] as well as irritable bowel syndrome [80]. Relationship between coffee/CAF consumption and colonic inflammation has been summarized in Table 1 [81-86].
An association between coffee/CAF consumption and colonic tumorigenesis has been summarized in Table 2 [87-102]. Within this table, about 84% of studies showed the beneficial effects of coffee/CAF intake for CRC development among the various type of studies. Still, the remaining less than 20% of studies show the opposite or inconclusive effects. In particular, high levels of coffee intake (more than 4 cups of coffee) reduce the risk of CRC recurrence and death in advanced CRC patients [99]. In contrast, high levels of coffee consumption are also associated with the initiation and promotion of CRC development but not associated with the incidence of earlier-stage cancers [49]. Overall, the relationship between coffee/CAF consumption and CRC incidence is largely variable [15] and we cannot explain the reasons logically at present.
ORAL ADMINISTRATION OF CAF WITH SUCROSE SEEMS TO HAVE A POTENT CARCINOGENIC EFFECT IN A MURINE MODEL OF CHRONIC COLITIS
To examine the physiological anti-inflammatory effects of CAF under chronic colitis in vivo, C57Bl/6N WT mice (female, 6-8 weeks old) were purchased from Kyudo Corporation (Tosu, Saga, Japan) and maintained under SPF conditions in the animal facility at Kurume University School of Medicine (Kurume, Fukuoka, Japan). The animal protocols (#2020-049, #2021-042, #2022-035) have been reviewed and approved by the Kurume University School of Medicine Subcommittee on Research Animal Care. Unexpectedly, these mice did not drink 2.5 mM CAF-contained water since CAF may stimulate nerve terminals in the tongue by activating mouse transient receptor potential A1, which results in some pain and bitter sensations in the mice [103]. To overcome the remarkable aversion to CAF-containing water, we diluted the concentration of CAF up to 0.17 mM with water and added 10% sucrose (Sigma-Aldrich, St. Louis, MO, USA). Because 2.5 mM CAF is almost equivalent to 3-5 cups of coffee, 0.17 mM CAF is equivalent to 0.2-0.4 cups of coffee. Surprisingly, this phenomenon was unobserved in our previous experiments performed at Massachusetts General Hospital (Boston, MA, USA) by utilizing C57Bl/6J WT mice (male, 6-8 weeks old), which were purchased from Jackson Laboratories [74]. We have not been able to determine whether the differential responsiveness to CAF is due to differences in mouse subtypes (C57Bl/6J versus C57Bl/6N) or to the housing environment in the US (Massachusetts General Hospital) versus Japan (Kurume University School of Medicine). In our previous experiment, we knew that a CAF concentration of less than 1 mM did not significantly influence CHI3L1 expression in SW480, a human colon cancer cell line [22]. The 0.17 mM CAF concentration we used in this current experiment is about 14.7 times less concentrated than 2.5 mM. It is suspicious that 0.17 mM CAF has enough effects in blocking the biological functions of the family 18 chitinase or affects their transcriptional expression levels compared to the former 2.5 mM CAF administrating experiment performed in 2013 [74].
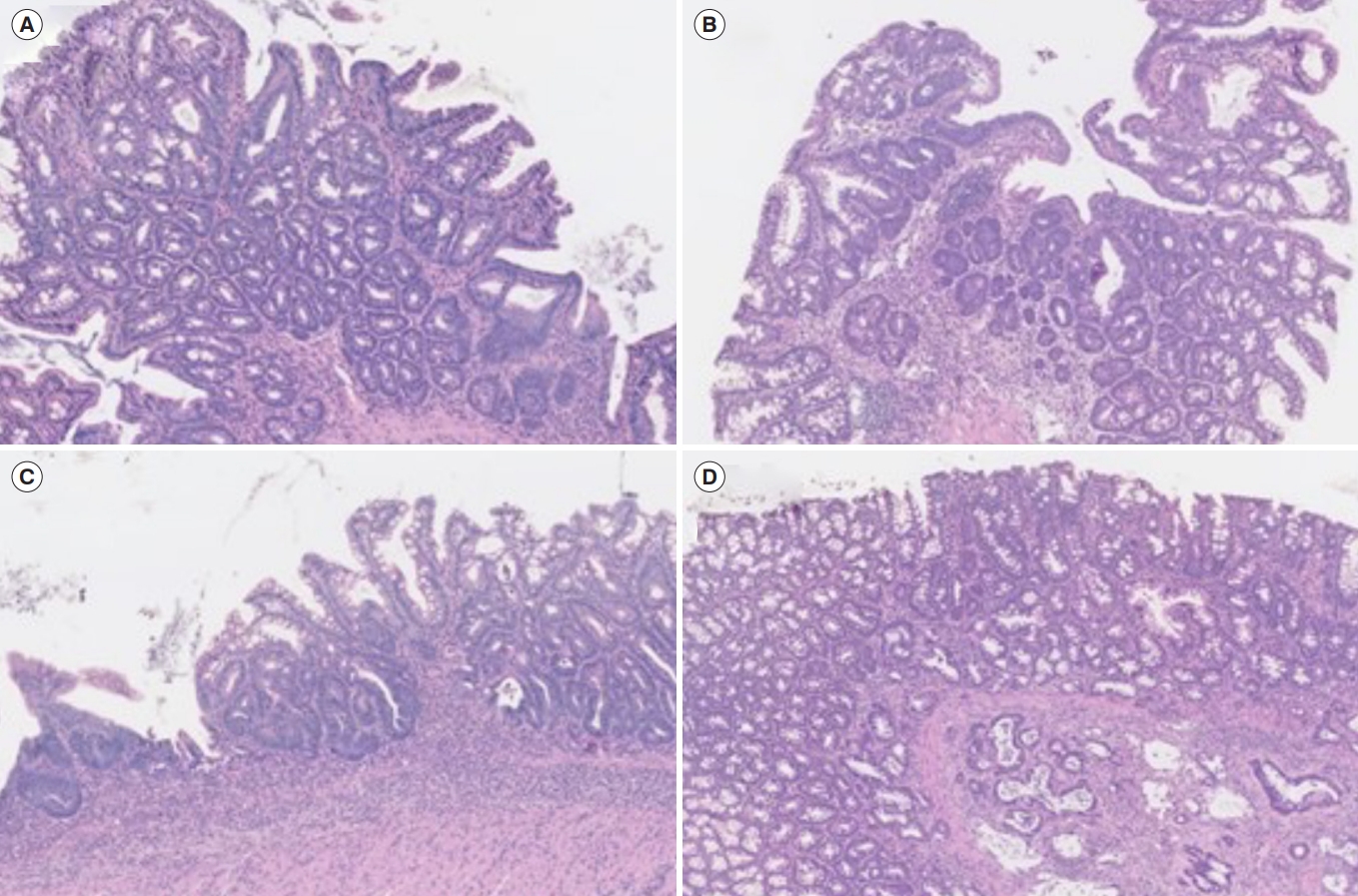
The chronic colitis was induced by the 3 cycles of 2.5% DSS administration. Briefly, mice were treated with 2.5% DSS in water for 4 days and then with 10% sucrose water with or without CAF or PTXN for the next 10 days for 3 cycles. After the 3rd cycle of DSS treatment, all the mice were treated with water without 10% sucrose. Diagnostic criteria for the tumors and colitis were described in Tables 3 and 4, respectively. In general, only 3 cycles of DSS treatments without pretreatment of azoxymethane, a carcinogenic reagent, in C57Bl/6N WT mice do not show carcinogenic changes in CECs. However, 6 out of 7 mice (85.7%) treated with 0.17 mM CAF with 10% sucrose developed dysplasia, carcinoma in situ, or invasive cancer. In contrast, none of the mice treated with 10% sucrose or 1.0 mM PTXN with 10% sucrose had any neoplastic changes in their CECs. Inflammatory scores determined by the hematoxylin and eosin sections are shown in Fig. 2. The average histological scores in 10% sucrose, CAF with 10% sucrose, and PTXN with 10% sucrose were 2.85, 8.42, and 4.3, respectively. This result suggests that low-dose CAF treatment with 10% sucrose induced severe inflammation accompanied by neoplastic changes in CECs during the DSS-induced chronic inflammation in mice. Surprisingly, 2 out of 7 (28.5%) showed carcinogenic changes of colonic epithelium after treatment with low-dose CAF with 10% sucrose after 3 cycles of DSS administration without azoxymethane treatment. Representative images of low-grade dysplasia (Fig. 2A), high-grade dysplasia (Fig. 2B), carcinoma in situ (Fig. 2C), and invasive carcinoma (Fig. 2D) in the low-dose CAF with 10% sucrose-treated mice have been shown.
Sucrose consists of fructose and glucose, and there are a couple of papers, which suggest that sucrose or fructose enhances intestinal tumor growth in the colon [104-106]. Further experiments would be required to monitor the exact serum concentration of CAF in the 3 (sucrose, glucose, or fructose-treated) groups in association with the expression of chitinase/CHI3L1 on CECs of mice more strictly. Sugar is commonly used as a sweetener for coffee and other caffeinated foods and beverages, and sucrose is the main component of sugar. For this reason, we urgently need to continue some selected biological and physiological experiments to prove the carcinogenic mechanisms under the additive effects of low-dose CAF and sucrose.
CONCLUSIONS
Coffee is one of the most frequently consumed beverages and is a complex of more than 1,000 bioactive compounds, including CAF. Of note, methylxanthine derivatives, including CAF, PTXN, and theophylline, are known as pan-chitinase inhibitors, which exert anti-inflammatory effects both in vitro and in vivo. In general, regular as well as large amounts of coffee consumption are believed to lower the risks of colonic inflammation and CRC mortality, and there are numerous reports on the relationship between coffee/CAF intake and CRC development. Unexpectedly, we have found that low-dose CAF with 10% sucrose (a major component of sugar) causes carcinogenic changes in CECs under chronic inflammatory conditions. Clarifying the anti-inflammatory as well as pro-tumorigenic mechanisms of CAF at the cellular levels could be the key to seeking more therapeutic as well as prophylactic options in IBD, colitis-associated cancer, and CRC development.