A pulmonary nodule in a patient with Crohn’s disease
Article information

Question: A 44-year-old man presented with lower abdominal pain and diarrhea. He denied any respiratory symptoms. He had a 7-year history of ileocolonic CD. His medication included infliximab and azathioprine for 5 years, and mesalazine for 6 years. Loss of response to infliximab had been noted. Physical examination showed a body temperature of 37.2°C and left lower quadrant tenderness. Abdominal CT scan for bowel evaluation disclosed incidentally a nodule measuring 12 mm in diameter in the right lung (Fig. A, arrow). Sputum cultures and cytology showed negative results. Tests for tumor markers, β-D-glucan, the purified protein derivative, and in vitro interferon-γ release assay were also negative. Both bronchoscopy and CT-guided percutaneous biopsy failed to diagnose the lesion. As the nodule grew and primary lung cancer was not ruled out, the lung mass was resected by video-assisted thoracoscopic surgery for definite diagnosis. Gross examination revealed a solid yellow-white nodule measuring 25×20 ×13 mm (Fig. B). What is the most likely diagnosis?
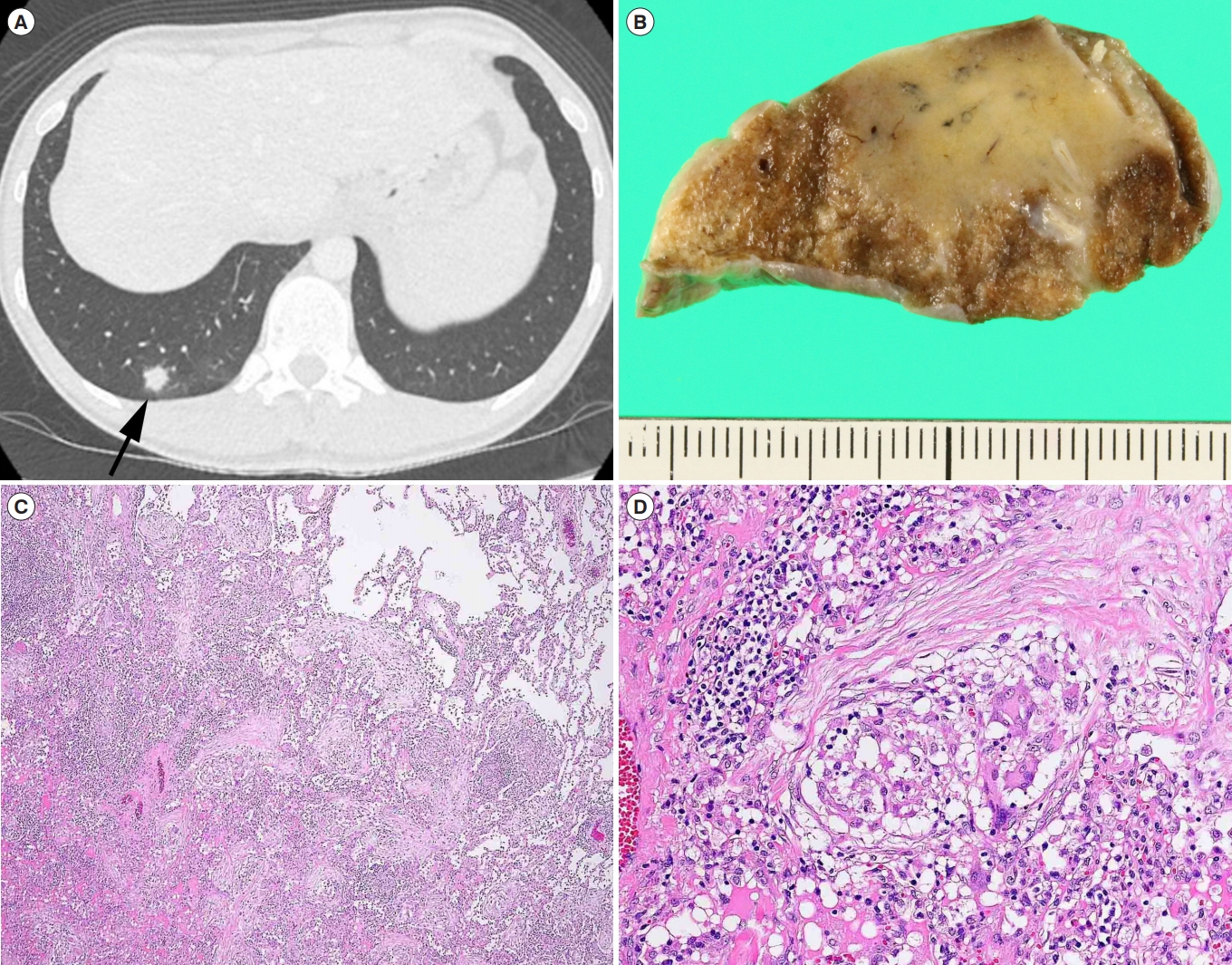
Answer to the Images: Pulmonary CD with Noncaseating Granulomas and Organizing Pneumonia
The pathological examination showed numerous noncaseating granulomas and organizing pneumonia (Fig. C, H&E, ×40). The granulomas contained typical multinucleated giant cells (Fig. D, H&E, ×200). Pulmonary CD with noncaseating granulomas and organizing pneumonia was diagnosed. Pulmonary lesions have not recurred during 2 years of follow-up with ustekinumab.
Bronchopulmonary involvement in CD is rare, but recently recognized as an important extraintestinal manifestation. These disorders consist of CD-related bronchopulmonary diseases, such as, organizing pneumonia, interstitial pneumonia, and granulomatous inflammation [1]. There may be a certain link between IBD and bronchopulmonary inflammation [2]. In cases of pulmonary granulomatous lesions in CD, mycobacterial or fungal infections under immunosuppressive therapy, and sarcoidosis should be excluded, as in this case.
Notes
FINANCIAL SUPPORT
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION
Collecting materials: Hokama A, Haranaga S, Ohira T, Iraha A, Kinjo T. Drafting the manuscript: Hokama A. Performing the surgery: Sasaki T. Examining the pathological findings: Matsumoto H. Reviewing the manuscript: Nahar S. Supervising the study: Fujita J. All authors reviewed the final version of the manuscript.