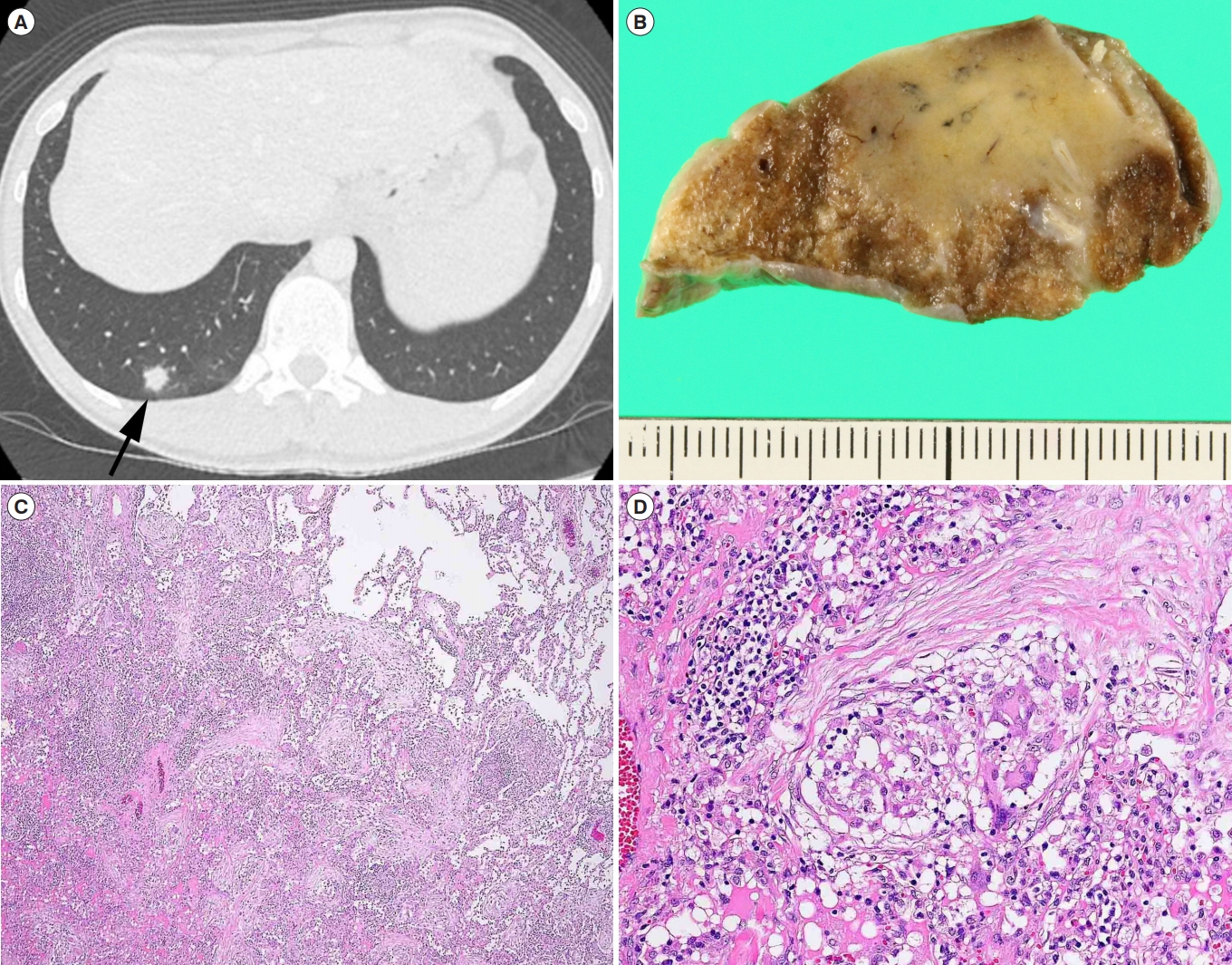
Question: A 44-year-old man presented with lower abdominal pain and diarrhea. He denied any respiratory symptoms. He had a 7-year history of ileocolonic CD. His medication included infliximab and azathioprine for 5 years, and mesalazine for 6 years. Loss of response to infliximab had been noted. Physical examination showed a body temperature of 37.2┬░C and left lower quadrant tenderness. Abdominal CT scan for bowel evaluation disclosed incidentally a nodule measuring 12 mm in diameter in the right lung (Fig. A, arrow). Sputum cultures and cytology showed negative results. Tests for tumor markers, ╬▓-D-glucan, the purified protein derivative, and in vitro interferon-╬│ release assay were also negative. Both bronchoscopy and CT-guided percutaneous biopsy failed to diagnose the lesion. As the nodule grew and primary lung cancer was not ruled out, the lung mass was resected by video-assisted thoracoscopic surgery for definite diagnosis. Gross examination revealed a solid yellow-white nodule measuring 25├Ś20 ├Ś13 mm (Fig. B). What is the most likely diagnosis?
Answer to the Images: Pulmonary CD with Noncaseating Granulomas and Organizing Pneumonia
The pathological examination showed numerous noncaseating granulomas and organizing pneumonia (Fig. C, H&E, ├Ś40). The granulomas contained typical multinucleated giant cells (Fig. D, H&E, ├Ś200). Pulmonary CD with noncaseating granulomas and organizing pneumonia was diagnosed. Pulmonary lesions have not recurred during 2 years of follow-up with ustekinumab.
Bronchopulmonary involvement in CD is rare, but recently recognized as an important extraintestinal manifestation. These disorders consist of CD-related bronchopulmonary diseases, such as, organizing pneumonia, interstitial pneumonia, and granulomatous inflammation [1]. There may be a certain link between IBD and bronchopulmonary inflammation [2]. In cases of pulmonary granulomatous lesions in CD, mycobacterial or fungal infections under immunosuppressive therapy, and sarcoidosis should be excluded, as in this case.