Laparoscopic surgery contributes to a decrease in short-term complications in surgical ulcerative colitis patients during 2008–2017: a multicenter retrospective study in China
Article information

Abstract
Background/Aims
The aim of this study was to analyze the chronological changes in postoperative complications in surgical ulcerative colitis patients over the past decade in China and to investigate the potential parameters that contributed to the changes.
Methods
Ulcerative colitis patients who underwent surgery during 2008–2017 were retrospectively enrolled from 13 hospitals in China. Postoperative complications were compared among different operation years. Risk factors for complications were identified by logistic regression analysis.
Results
A total of 446 surgical ulcerative colitis patients were analyzed. Fewer short-term complications (24.8% vs. 41.0%, P=0.001) and more laparoscopic surgeries (66.4% vs. 25.0%, P<0.001) were found among patients who received surgery during 2014–2017 than 2008–2013. Logistic regression suggested that independent protective factors against short-term complications were a higher preoperative body mass index (odds ratio [OR], 0.870; 95% confidence interval [CI], 0.785–0.964; P=0.008), laparoscopic surgery (OR, 0.391; 95% CI, 0.217–0.705; P=0.002) and elective surgery (OR, 0.213; 95% CI, 0.067–0.675; P=0.009). The chronological decrease in short-term complications was associated with an increase in laparoscopic surgery.
Conclusions
Our data revealed a downward trend of short-term postoperative complications among surgical ulcerative colitis patients in China during the past decade, which may be due to the promotion of minimally invasive techniques among Chinese surgeons.
INTRODUCTION
Ulcerative colitis (UC) is an immunologically mediated bowel disorder that progressively and chronically damages the colon and rectum [1]. Although medical treatment, including glucocorticoids and biological agents, has led to higher rate of disease remission [2] and lower rate of colectomy in recent years, 8% to 24% of UC patients still need surgical management [3,4].
Restorative total proctocolectomy with ileal pouch anal anastomosis (IPAA) is a theoretically curative and sphincter-preserving procedure that was first reported in 1978 by Parks and Nicholls [5], and this procedure has been internationally accepted as the gold standard for most surgical UC patients at present. The first reported total proctocolectomy plus IPAA for UC patients in China was in 1999 [6], and several studies have explored the clinical parameters impacting postoperative complications [7-9].
As biologic agents have emerged for treating UC patients, some studies revealed that the emergent colectomy rate and postoperative complications in acute severe UC have decreased [10,11], although some other studies held opposite opinion [12,13]. However, the reasons for the improved outcomes of UC surgery in the new era remain unclear. In addition, minimally invasive surgeries and individual IPAA stage procedures have been applied to improve surgical outcomes of UC patients [14,15]. However, surgeons still have concerns about whether IPAA surgery would increase postoperative complications, and whether the introduction of surgical techniques such as laparoscopic surgery and 3-stage IPAA procedures would contribute to favorable outcomes for UC patients.
Therefore, we retrospectively analyzed the trend of postoperative complications for surgical UC patients during 2008–2017 at 13 inflammatory bowel disease (IBD) centers throughout China, and the clinical parameters that contributed to the changes were investigated.
METHODS
1. Study Subjects
Details of the 13 IBD centers are listed in the acknowledgment section. UC patients who underwent colectomy from January 2008 to December 2017 were retrospectively enrolled. The inclusion criteria were a clinical and pathological diagnosis of UC and undergoing colectomy because of an emergency or an elective indication. The exclusion criteria were lost to follow-up and lacking important complication data. This study was approved by the Institutional Review Board of the Sixth Affiliated Hospital of Sun Yat-sen University (IRB No. 2019ZSLYE-197). All the methods were performed in accordance with the Declaration of Helsinki. Informed consent was not obtained from all the participants, and the need for consent of this study was deemed unnecessary by the Institutional Review Board of the Sixth Affiliated Hospital of Sun Yat-sen University according to national regulations.
2. Definitions of the Parameters
Patient characteristics, including age, sex, disease extent and severity, the preoperative body mass index (BMI), albumin, C-reactive protein, and erythrocyte sedimentation rate, were collected. Details on surgical methods, operation year, operative approaches (open or laparoscopic), surgical procedures (2-stage or 3-stage IPAA), and surgical complications were retrieved.
The disease extent of the UC patients was defined by the maximal macroscopic extent on colonoscopy and was classified as proctitis (E1), left-side colitis (E2), or extensive colitis (E3) according to the Montreal classification [16]. Disease severity was defined based on the Truelove and Witts classification, including an assessment of bloody stool, pulse, temperature, hemoglobin, C-reactive protein, and erythrocyte sedimentation rate level [17]. Surgical methods were defined as an IPAA procedure (hand sewn or stapled) and sub/total proctocolectomy with ileorectal or ileoanal anastomosis, sub/total proctocolectomy with ileostomy, or segmental colectomy and diverting loop ileostomy without bowel resection, which were grouped as non-IPAA procedures. The operation year was defined as the time when the patients received the first-stage operation. Detailed definitions of the surgery timing (emergency or elective), operative approaches, and surgical stage of the IPAA are shown in Supplementary Table 1.
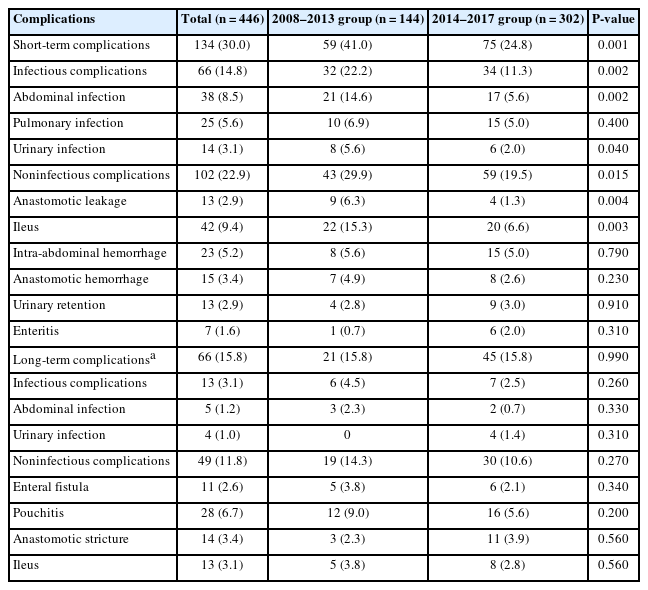
Comparison of Postoperative Complications in Patients with Ulcerative Colitis between Subgroups of 2008–2013 and 2014–2017
3. Outcome Measurement
The primary outcome of this study was postoperative complications, including short-term and long-term complications. Short-term complications were defined as complications that occurred within 30 days after any stage of the operation, including intra-abdominal hemorrhage (requiring blood transfusion or an invasive intervention), abdominal infection, ileus, pulmonary infection, urinary retention, urinary infection, anastomotic leakage, anastomotic hemorrhage, and enteritis. Longterm complications were defined as complications that occurred more than 30 days after any stage of the operation, which included anastomotic stricture (requiring instrumental dilatation or surgical intervention), pouchitis, abdominal infection (including abscess), enteral fistula, ileus, and urinary infection. We categorized complications into infectious and noninfectious complications basing on whether they were caused by definite pathogenic microorganism. More detailed definitions of the complications are shown in Supplementary Table 1.
4. Statistical Methods
Continuous variables are presented as the mean ± standard deviation (SD) or median (range), and categorical data are presented as numbers (percentages). Student t-tests and Mann-Whitney U tests were used to compare continuous variables, and chi-square tests were used to compare categorical variables. Linear-by-linear associations test was used to assess the chronological changes in postoperative complications. Univariate and multivariable logistic regression models were used to identify the risk factors for postoperative complications. Statistical analyses were performed with SPSS software version 19.0 (IBM Corp., Armonk, NY, USA). A P-value <0.05 was considered statistically significant.
RESULTS
1. Short-term Complications for Surgical UC Patients Decreased during 2008–2017
A total of 446 UC patients who received surgical treatment during 2008–2017 were enrolled, with a mean age of 44.7 ± 14.2 years, and 58.7% of them were men. The five most common indications for surgical treatment were: ineffective medical therapy (63.5%), uncontrolled intestinal bleeding (11.6%), patients’ personal demand (11.0%), dysplasia or cancer (5.7%), and toxic megacolon (4.1%). The number of surgical UC patients in China increased after 2013 (Supplementary Fig. 1). A total of 134 cases (30.0%) of short-term complications and 66 cases (15.8%) of long-term complications were observed after a follow-up of 30.1 months (range, 1.0–125.9 months). As shown in Fig. 1, the incidence of short-term complications in surgical UC patients showed a significant downtrend (P<0.001), while the similar trend was not observed for the incidence of long-term complications.
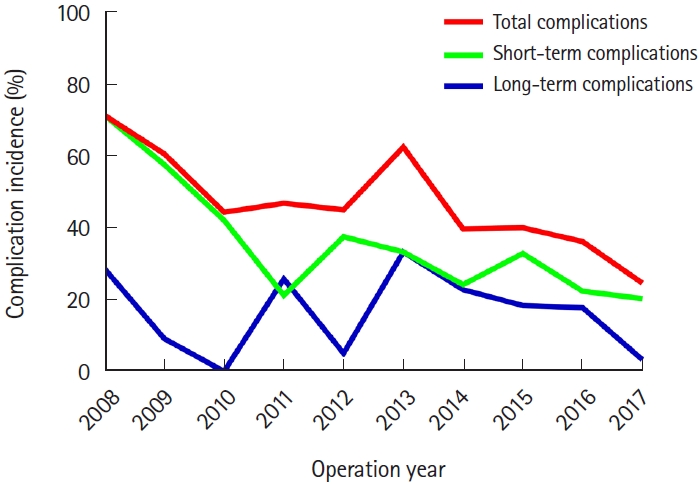
Chronological change of postoperative complications including total complications, short-term complications, and long-term complications for surgical ulcerative colitis patients during 2008–2017 in China.
Considering that laparoscopic surgery has become popular in China since 2014, we divided the patients into 2007–2013 and 2014–2017 subgroups according to their operation year. As shown in Table 1, patients who underwent surgery during 2014–2017 had lower rates of short-term complications, infectious short-term complications, abdominal infections, anastomotic leakage, urinary infections, and ileus (all P<0.05). No significantly difference of long-term complications including pouchitis was found between the 2007–2013 and 2014–2017 subgroups (P>0.05).
2. Higher BMI, Elective Surgery and Laparoscopic
Surgery Protect against Short-term Complications Clinical parameters were compared among patients with and without short-term postoperative complications. As shown in Table 2, patients who had short-term postoperative complications were characterized by more E1 disease (12.3% vs. 4.4%, P=0.025), a lower preoperative BMI (18.8 ± 2.7 kg/m2 vs. 20.1 ± 3.1 kg/m2, P=0.003), and underwent more open surgery (57.5% vs. 42.4%, P=0.004) and emergency surgery (17.1% vs. 7.2%, P=0.001).

Compared of Clinical and Surgical Parameters between Surgical Ulcerative Colitis Patients with and without Short-term Postoperative Complications
Logistic regression analysis was performed to explore risk factors for short-term complications of surgical UC patients. As shown in Table 3, a higher preoperative BMI (odds ratio [OR], 0.864; 95% confidence interval [CI], 0.783–0.954; P=0.004), laparoscopic surgery (OR, 0.546; 95% CI, 0.362–0.822; P=0.004), and elective surgery (OR, 0.366; 95% CI, 0.196–0.684; P=0.002) were protective factors against short-term complications in UC patients who underwent surgery, according to the univariate logistic regression analysis. After adjusting for confounding factors, including preoperative BMI, operative approach (laparoscopy vs. open surgery), surgery timing (elective vs. emergency) and operation method (non-IPAA vs. IPAA), multivariable logistic regression analysis showed that independent protective factors for short-term complications were a higher preoperative BMI (OR, 0.870; 95% CI, 0.785–0.964; P=0.008), laparoscopic surgery (OR, 0.391; 95% CI, 0.217–0.705; P=0.002) and elective surgery (OR, 0.213; 95% CI, 0.067–0.675; P=0.009).

Univariate and Multivariable Logistic Regression Analyses of Risk Factor for Short-term Complications in Surgical Ulcerative Colitis Patients
3. The Decrease in Short-term Complications Was Associated with Laparoscopic Surgery
We then compared clinical and surgical characteristics between patients who received surgery during 2008–2013 and 2014–2017. As shown in Table 4, more men (62.6% vs. 50.7%, P=0.020), more laparoscopic surgery (66.4% vs. 25.0%, P<0.001) and more 3-stage IPAA procedures (27.8% vs. 10.6%, P=0.002) were found in patients who underwent surgery during 2014–2017. Then, patients were divided into IPAA and non-IPAA cohorts, and the complications were compared (Table 5). For patients who received IPAA surgery, the difference in overall short-term postoperative and short-term infectious complications between open surgery and laparoscopic surgery was statistically significant (short-term complications, P<0.001; infectious complications, P=0.009), while among patients who received non-IPAA surgery, the benefit of laparoscopic surgery was not statistically significant (P>0.05).

Compared of Clinical and Surgical Parameters between Surgical Ulcerative Colitis Patients Received Operation during 2008–2013 and 2014–2017
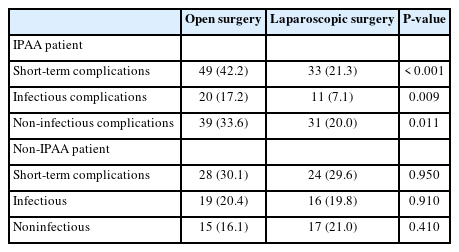
Compared of Short-term Postoperative Complications in Surgical Ulcerative Colitis Patients between Subgroups of Open Surgery and Laparoscopic Surgery
DISCUSSION
In this article, we analyzed the chronological changes in postoperative complications for surgical UC patients during 2008–2017, and it was revealed that short-term complications, including infectious complications, decreased in the past decade in China. The decrease in complications was consistent with the increased application of laparoscopic surgery. Logistic regression analysis revealed that laparoscopic surgery was an independent protective factor for short-term postoperative complications.
The incidence of UC in China has increased, with a current incidence of 0.42 per 1,000,000 person-years [18]. To our knowledge, this retrospective study is the first published nationwide multicenter investigation on surgical treatment of UC in China. As the IBD centers developed in China, more and more UC patients were diagnosed and managed by medical treatments and operations. Our results showed that the number of patients who underwent surgery increased after 2014, but the short-term postoperative complications among surgical UC patients decreased. Although postoperative complications were variable over time and geographical area in previous studies, the risk of postoperative complications for UC patients worldwide has decreased in recent decades [19,20]. A systematic review including UC patients from China suggested that postoperative complications improved after 2010, but the author did not investigate the possible factors causing this effect [21].
Recently, there has been some concern that complications among UC patients who receive IPAA procedures may be affected by the introduction of biological reagents such as infliximab or vedolizumab, although this issue remains controversial [22]. Preoperative corticosteroid treatment was regarded as a risk factor for postoperative complications for IBD patients [23], and according to our investigation, preoperative treatment with glucocorticoids did not increase the risk of postoperative complications. This might be due to the individual surgical management such as avoiding emergent IPAA operation and effective rescue therapy for patients who received high-dose corticosteroid treatment. As the introduction of infliximab for moderate-severe active UC into China in 2007, more than 10% of surgical patients from this study received anti-tumor necrosis factor agents before surgery, and it was suggested that preoperative infliximab treatment did not affect the postoperative complications, which was been proved previously [24]. Lower BMI was found to be an independent risk factor for short-term complications in surgical UC patients, while it was reported that higher BMI was associated with frequent complications in patients receiving IPAA procedure [25]. According to our data, approximately 60% of UC patients had a BMI of < 20 kg/m2. Obesity did not become a routine problem for UC patients in China. On the contrast, lower BMI appeared to increase complications in surgical UC patients. This clinical feature was quite different between Asia and Caucasian patients.
Laparoscopic surgery was a significant factor that contributed to the decline in postoperative complications. Our previous meta-analysis concluded that UC patients who underwent laparoscopic surgery had a lower total complication rate, although laparoscopic surgery prolonged the operation duration [26], and it has already been widely accepted that the laparoscopic approach is associated with fewer complications and lower morbidity and mortality [27]. Moreover, this minimally invasive technique resulted in favorable long-term outcomes for UC patients, including fewer complications and a more balanced emotional condition [28]. The popularization of laparoscopic techniques for Chinese UC patients has helped improves their surgical outcomes. On the other hand, the benefit of laparoscopic surgery was only found to be statistically significant in the IPAA surgery subgroup, while among patients who received non-IPAA surgery, laparoscopic surgery did not reduce postoperative complications. Due to the technically demanding IPAA surgery and concerns about its risks of complications, colorectal surgeons do not perform IPAA surgery for all UC patients. The advantage of laparoscopic surgery for IPAA surgery includes a better view of the pelvis, neural preservation, and a clear anastomosis, and our results support the advantages of using laparoscopic surgery for IPAA.
The 3-stage IPAA, defined as subtotal colectomy and followed by excising remaining rectum and IPAA at the second time, and finally close ileostomy, was regards as a safer procedure for high-risk surgical UC patients [29]. In our data, similar short-term complications were found between subgroups of 2-stage and 3-stage IPAA procedures. However, the patients who received the 3-stage IPAA procedure in this study were more likely to be at high risk for short-term complications, including a lower BMI, more preoperative infliximab treatment and more emergency operations (data not shown). This result is consistent with the conclusion by Mège et al. [29] and indicated that the 3-stage IPAA procedure is safer for patients with acute severe disease, although some other studies suggested that 2-stage IPAA also appeared to be safe and appropriate even for high-risk patients [30]. Therefore, the issue concerning IPAA stage still needs to be investigated in prospective research in the future.
No significant difference in long-term complications including pouchitis was found in the chronological analysis. According to Table 4, gender, operation approach and IPAA stage were significant variables between 2008–2013 and 2014–2017 subgroups. It was reported that 3-stage IPAA and biologic agents were protective against long-term complications such as pouchitis and septic complications [31], while those complications did not show significant difference in our data although more 3-stage IPAA procedures were operated in the later years. Moreover, long-term complication information was lost in the 29 cases (6.5%) of overall patients. Thus, the change of the long-term complication needs to be investigated as more biological agents would be used in the future.
Our study has a few limitations. First, this is a multicenter retrospective study, and heterogeneity of the patient characteristics and surgical methods was inevitable. Second, long-term outcomes such as surgical failure, quality of life, and sexual function were not investigated in this study due to insufficient follow-up time, and the long-term cancer rate of the residual rectum or pouch is unknown. Further investigation is necessary. Third, we did not identify institutional or individual learning curves or surgeon/hospital volumes in this study, and the exact influence of surgical techniques from various surgeons on the outcome of surgical UC patients also needs to be determined.
Above all, our data revealed a downward trend of short-term postoperative complications among surgical UC patients in China during the past decade, which may be due to the promotion of minimally invasive techniques among Chinese surgeons.
Notes
Funding Source
This work was supported by National Natural Science Foundation (grant number 81800484), Science & Technology Planning Project of Guangdong Province (grant numbers 20160916, 2015B020229001) and National Key Clinical Discipline in general surgery.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability Statement
Not applicable.
Author Contributions
Conceptualization: Cai Z, He Z, Lan P, Wu X. Data curation: Cai Z, He X, Gong J, Du P, Meng W, Zhou W, Jiang J, Wu B, Yuan W, Xue Q, Yuan L, Wang J, Tai J, Liang J, Zhu W. Funding acquisition: Cai Z, Lan P, Wu X. Investigation: Cai Z, He X. Methodology: Cai Z, He X. Writing - original draft: Cai Z. Writing - review & editing: all authors. Approval of final manuscript: all authors.
Additional Contributions
Collaborative IBD centers are as follows: Jinling Hospital (Nanjing University), Xinhua Hospital (Shanghai Jiao Tong University), West China Hospital (Sichuan University), the Sixth Affiliated Hospital (Sun Yat-sen University), Sir Run Run Shaw Hospital (Zhejiang University), the First Affiliated Hospital (Zhejiang University), Qilu Hospital (Shandong University), Peking Union Medical College Hospital, the First Affiliated Hospital (Zhengzhou University), Nanfang Hospital (Southern Medical University), the Second Xiangya Hospital (Central South University), First Hospital (Jilin University), and Xijing Hospital (Fourth Military Medical University).
We thank Lei Lian, Xianrui Wu, Bin Zheng, Xuanhui Liu, Xuming Huang, Wenyu Li, Xiaoling Li, and Futian Luo for their assistance in the study.
Supplementary Material
Supplementary materials are available at the Intestinal Research website (https://www.irjournal.org).
Supplementary Fig. 1. Chronological change of surgical ulcerative colitis (UC) patients in numbers during 2008–2017 in China.
ir-2022-00012-suppl1.pdfSupplementary Table 1. Definitions and Diagnostic Criteria for Surgical Characteristics and Complications
ir-2022-00012-suppl2.pdf