Sedation for routine gastrointestinal endoscopic procedures: a review on efficacy, safety, efficiency, cost and satisfaction
Article information
Abstract
Most gastrointestinal endoscopic procedures are now performed with sedation. Moderate sedation using benzodiazepines and opioids continue to be widely used, but propofol sedation is becoming more popular because its unique pharmacokinetic properties make endoscopy almost painless, with a very predictable and rapid recovery process. There is controversy as to whether propofol should be administered only by anesthesia professionals (monitored anesthesia care) or whether properly trained non-anesthesia personnel can use propofol safely via the modalities of nurse-administered propofol sedation, computer-assisted propofol sedation or nurse-administered continuous propofol sedation. The deployment of non-anesthesia administered propofol sedation for low-risk procedures allows for optimal allocation of scarce anesthesia resources, which can be more appropriately used for more complex cases. This can address some of the current shortages in anesthesia provider supply, and can potentially reduce overall health care costs without sacrificing sedation quality. This review will discuss efficacy, safety, efficiency, cost and satisfaction issues with various modes of sedation for non-advanced, non-emergent endoscopic procedures, mainly esophagogastroduodenoscopy and colonoscopy.
INTRODUCTION
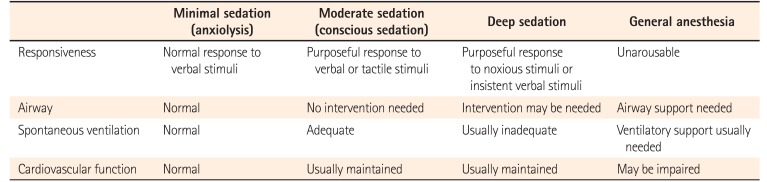
In developed countries, the majority of routine, low-risk endoscopic procedures are currently performed with some form of sedation.1 Gastrointestinal (GI) endoscopy is an inherently uncomfortable procedure, with the potential for abdominal pain, cramping and bloating during colonoscopy,2 and gagging, retching and choking during esophagogastroduodenoscopy (EGD). The use of sedation allows for a more thorough and relaxed procedure, with higher polyp detection rates and procedures completion rates.3 A sedated, comfortable patient not only enhances endoscopist satisfaction,4 but is associated with a higher likelihood of the patient being willing to undergo the procedure again. The American Society of Anesthesiology (ASA) has published definitions for different levels of sedation (Table 1);5 specifically, at the level of “moderate sedation,” the patient maintains ventilatory and cardiovascular function and is able to make purposeful responses to verbal or tactile stimuli, while at “deep sedation,” patients cannot be easily aroused but is still able to respond to noxious or insistent stimuli. Airway support may be required for deep sedation. To allow the procedure to proceed smoothly, sedatives are usually dosed to achieve moderate sedation (benzodiazepine and opiate sedation) or deep sedation (monitored anesthesia care with propofol). In a minority of cases, full “general anesthesia” (with intubation of the patient and the use of anesthetic agents such as nitrous oxide or ketamine) is required because of patient characteristics or procedural complexity. Since full general anesthesia is not commonly used for routine GI endoscopy, it will not be discussed further in this review.

NON-SEDATED ENDOSCOPY
Although sedation for endoscopy is becoming widespread, there is still interest in non-sedated endoscopy, even in countries like the United States where almost all GI procedures are performed with sedation. Non-sedated endoscopy offers several potential advantages−lower cost, wider availability, less risk, higher efficiency and decreased post-procedural impairment, allowing for patients to drive or return to work immediately afterwards. There continue to be attempts to develop unsedated EGD using ultrathin transnasal endoscopes,6 and unsedated colonoscopy using water immersion techniques.7 Motivated patients can successfully undergo unsedated endoscopy,8 but the vast majority of patients in developed countries prefer and demand sedation, and the overall trend in GI endoscopy is moving towards more potent, not less potent, forms of sedation.910
MODERATE SEDATION WITH SEDATIVES, HYPNOTICS AND OPIOIDS
Initial forms of sedation for GI endoscopy involved moderate sedation using such agents as midazolam, diazepam, pethidine, fentanyl, remifentanil and/or meperidine. Midazolam and diazepam are intravenous benzodiazepines, with powerful sedative, anxiolytic, hypnotic and amnestic effects. Fentanyl, remifentanil and meperidine are intravenous opioid analgesics, with only minimal sedative effects. Typically, moderate sedation is induced by a combination of a benzodiazepine sedative and an opioid analgesic, which have complementary and synergistic effects with each other. Midazolam and fentanyl (MF) have now become the most commonly used moderate sedation agents in the United States,11 and many other countries.12 Even though some studies reported similar efficacy for midazolam and diazepam,13 midazolam is now usually favored over diazepam because of its faster onset of action and better safety profile,1415 while fentanyl has now supplanted meperidine because the former is associated with more rapid onset and clearance, with less nausea.1617 Midazolam is a water-soluble compound prepared in an acidic solution. After introduction into the bloodstream, it reconfigures to a lipophilic structure at physiological pH, rapidly diffusing across the blood-brain barrier into the CNS. The usual total dose for GI endoscopy is 2 to 10 mg. Fentanyl, a synthetic opioid agonist with powerful analgesic but only mild sedative properties, is highly lipid soluble and 80 times more potent than morphine. The usual total dose is 50 to 200 µg. Both agents have a relatively fast onset of action when given intravenously and a short duration of effect (Table 2). Effective reversal agents, naloxone for opioids and flumazenil for benzodiazepines, are readily available. In addition to MF, ancillary agents such as diphenhydramine or droperidol are sometimes used. These agents potentiate the actions of the primary benzodiazepine/opioid regimen, and may be needed for patients who are unusually difficult to sedate. The use of droperidol has been limited by its cardiac risks, especially in patients with a history of prolonged QT intervals or electrolyte abnormalities.

Properties of Commonly Used Sedative Agents for Gastrointestinal Endoscopy
Monitoring during sedated endoscopy typically involves assessment of the electrocardiogram (EKG) pattern, blood pressure, pulse oximetry and patient responsiveness;17 in many units, capnography is also used, particularly with propofol sedation. Experimental methods such as bispectral index monitoring, a form of electroencephalography, are not widely available as yet.
MF sedation has been found to be effective for routine GI endoscopy.18 The safety profile for MF compares quite favorably to that of propofol. Studies have shown that the cardiopulmonary complication rates with MF sedation are generally low, between 0.05% to 0.10% for EGDs and colonoscopies.17 A recent meta-analysis of 27 studies (many of them randomized controlled trials) found that propofol was associated with similar risks of hypoxia (OR, 0.82; 95% CI, 0.63−1.07), and hypotension (OR, 0.92; 95% CI, 0.64−1.32) as MF or other traditional sedative agents; for non-advanced procedures, propofol was slightly less likely to cause complications (OR, 0.61; 95% CI, 0.38−0.99).19
MONITORED ANESTHESIA CARE
The administration of propofol by anesthesia professionals in order to induce deep sedation in unintubated patients is termed “monitored anesthesia care (MAC)” and is one of the most common sedation methods for GI procedures in North America and Europe. Propofol (2,6-diisopropyl phenol) is a short-acting agent with sedative, amnestic and hypnotic properties. It is not an analgesic, but has synergistic effects when given with opioids or benzodiazepines. The target entity is the type A γ-aminobutyric acid receptor. A typical preparation consists of a 1% solution, prepared in a mixture of soybean oil, glycerol and egg lecithin, hence it is contraindicated in patients with soy or egg allergy. Propofol, a highly lipophilic compound, is 98% plasma-protein bound, and is metabolized in the liver by conjugation to glucuronide sulfate to produce water-soluble metabolites excreted by the kidneys. The time from injection to onset of sedation is 30 to 60 seconds, and its duration of effect is 4 to 8 minutes, although its duration of peak effect is considerably shorter (often 1−2 minutes). Its pharmacokinetics do not change in patients with renal or liver failure (Table 2). Because it reduces cardiac output and systemic vascular resistance, it often causes hypotension, while its sedative effects can lead to hypoventilation. Propofol can also cause pain at the injection site, but it is rare for phlebitis to occur.
1. Effectiveness and Safety Data
Propofol does not have any known reversal agent, but its extremely short half-life enhances its safety profile considerably. Propofol sedation is associated with relatively good cognitive function in the recovery period,2021 and driving and psychomotor skills recover rapidly,22 in contrast to MF sedation.23 There have been numerous randomized controlled trials comparing propofol against MF sedation for GI procedures; these data have been summarized in several meta-analyses. Generally, the studies show that propofol is extremely effective at inducing adequate procedural sedation, with high procedural success rates, rapid recovery times and low complication rates. One of the earliest meta-analyses combined data from 12 studies, concluding that propofol for colonoscopy had lower odds of cardiopulmonary complications compared with traditional agents, but for other procedures, the complication risks were similar.24 A subsequent meta-analysis of 36 randomized studies showed that compared with MF, propofol expeditiously induced deeper sedation, with high patient satisfaction, and faster and more predictable recovery.18 Another meta-analysis that included 22 randomized controlled trials found that propofol was associated with better patient cooperation, shorter recovery and discharge times, higher post-sedation recovery scores and better sedation.25 Finally, a meta-analysis of 5 studies on propofol sedation for EGDs in cirrhotic patients showed that propofol led to more rapid sedation and recovery than MF, but the risk of sedation-related side effects did not differ significantly.26
2. Prevalence of Use
In the United States, where the vast majority of propofol sedation is currently administered by anesthesia professionals, the use of propofol has been fraught with controversy, primarily around the issues of reimbursement and privileging. Over the span of a decade, there has been a 3- to 4-fold increase in the prevalence of anesthesia involvement in routine outpatient endoscopic procedures on low-risk patients, with propofol sedation rates going from 14% in 2003 to 48% in 2013 for Medicare patients, and from 14% in 2003 to 53% in 2013 for privately insured patients.9102728 Canada has also seen analogous increases.29 This has led to significant increases in anesthesia costs for GI endoscopy.3031 Against the current background of national concern about burgeoning health care costs, there is evidence that a large proportion of MAC use is medically unnecessary because they involve low-risk procedures that can presumably be performed with moderate sedation using MF or other traditional agents. Furthermore, there are dramatic regional variations in the use of MAC (with the highest rates in areas like New York and Florida), which further supports the notion that much of MAC use is discretionary and redundant.432
3. Problems
The use of anesthesiologist-administered propofol for low-risk endoscopies is estimated to cost the U.S. health care system an additional $3.2 billion (USD) over a period of 10 years.31 Although it is somewhat difficult to define “discretionary” anesthesia care with exactitude,33 there are widespread concerns that these substantial anesthesia costs are not justified by any improvement in clinical outcomes.34353637 Firstly, the use of MAC does not increase the adenoma or polyp detection rate during colonoscopy.303839 Furthermore, anesthesia-administered propofol sedation may not necessarily be safer than non-anesthesiologist administered MF sedation. Although the use of MAC does not seem to be associated with higher perforation rates,4041 studies looking specifically at force application during colonoscopy found that axial and radial forces tend to be stronger because the patient is more heavily sedated.42 In fact, available data either show similar complication rates,253243 or higher complication rates with MAC compared with MF sedation.444546 Since none of these studies were randomized, there are legitimate concerns about selection bias, but it is clear that currently available data do not support the notion that anesthesia-administered propofol is safer than MF sedation.3536
NURSE ADMINISTERED PROPOFOL SEDATION
Because of these issues with MAC, there have been attempts to investigate nurse-administered propofol sedation (NAPS).47 The NAPS dosing protocol varies between centers and countries. In the United States, specially trained nurses typically administer small boluses of propofol at frequent intervals to achieve moderate sedation. In most cases, an initial bolus of 30 to 50 mg is given through a rapidly running intravenous line, followed by boluses of 10 to 20 mg every 30 to 60 seconds.48 The use of NAPS instead of MAC for low-risk patients undergoing routine GI procedures seems to represent “low lying fruit” for cost savings and better resource allocation,49 but NAPS has remained one of the most controversial aspects of the GI field.3435 European and American GI guidelines endorse the use of NAPS for low-risk GI procedures, provided that practitioners undergo proper training.505152 However, these guidelines are at odds with those issued by the ASA, which states that clinicians who use propofol “should be qualified to rescue patients from any level of sedation including general anesthesia.”53
1. Effectiveness and Safety Data
Numerous studies from Europe and America have shown NAPS to be feasible and safe, as long as it is performed on appropriately selected patients.545556575859 Contraindications to NAPS include the presence of significant comorbidities (ASA class 3 or above), severe sleep apnea, morbid obesity, gastric outlet obstruction, gastroparesis and achalasia; patients undergoing advanced complex endoscopic procedures may also be unsuitable for NAPS.48 Direct comparisons have shown that NAPS is associated with higher patient satisfaction scores and shorter recovery times compared with MF sedation.58 Randomized controlled studies show that NAPS is associated with fewer adverse events and higher satisfaction scores than MAC.60 Generally, NAPS seems to be more easily used for colonoscopy than EGD, with a lower risk of having to resort to mask ventilation.5961 An exhaustive review of worldwide safety data involving 646,080 NAPS procedures reported only 11 emergent endotracheal intubations, no permanent neurological injuries and 4 deaths; only 0.1% of patients required transient mask ventilation.55
2. Regulatory and Financial Obstacles
NAPS is used extensively in several European countries, including Germany, Sweden, and Switzerland.5062 Payment models seem to have a marked impact on whether anesthesia-administered propofol or NAPS is used; in countries where separate anesthesia service fees are charged (such as France), anesthesia-administered propofol is the dominant model, whereas in other countries NAPS is more popular.63 In the United States, NAPS is rarely used.64 In addition to financial issues, there are other barriers to its use in the United States, including the U.S. Food and Drug Administration labeling for propofol (which specifies that propofol must be administered by personnel trained in anesthesia), policies of the U.S. Center for Medical Services (the government entity that administers Medicare) on deep sedation, insurance regulations, hospital credentialing rules, and medicolegal concerns.6465 Many U.S. institutions that previously performed many cases with NAPS, such as the University of Indiana, have now abandoned its use because of insurmountable regulatory and medicolegal obstacles.64
PATIENT CONTROLLED SEDATION
Patient controlled sedation (PCS) is analogous to the patient-controlled analgesia used in hospitals, where patients can control their own dosage of pain medications. PCS has been looked at in several studies and found to be effective compared against MAC66 and conventional MF-type sedation.676869 However, PCS is not widely used because most patients are reluctant to take charge of their own sedation.
COMPUTER-ASSISTED PROPOFOL SEDATION
The SEDASYS® System (Ethicon Endo-Surgery, Inc., Cincinnati, OH, USA) was approved in the United States in 2013 for providing moderate sedation for ASA class 1 and 2 patients undergoing routine EGD and colonoscopy. Despite considerable media attention, there still seem to be some misconceptions about this technology. SEDASYS® is not a “robotic anesthesiologist.” It is a system with built-in safeguards to allow trained non-anesthesiologist physicians on-label access to propofol. Also, SEDASYS® is not a “closed-loop” system. Depending on patient vital signs, the system may restrict, suspend, decrease or stop the propofol infusion, but any increase in drug delivery must be initiated by the clinician. Finally, SEDASYS® is not a “target controlled” system and does not control delivery based on the propofol concentration in the plasma or at the site of drug effect.
1. Mechanics
Computer-assisted propofol sedation (CAPS) allows non-anesthesiologists to administer 1% propofol as a continuous infusion after a premedication dose of fentanyl of 25 to 100 µg. The initial infusion rate is determined by the endoscopist and can range from 25 to 75 µg/kg/min. To achieve a suitable level of sedation, the endoscopist can titrate the maintenance infusion rate upwards or downwards during the procedure. A bolus dose of up to 0.25 mg/kg can also be given.
The CAPS system continuously monitors capnography, oxygen saturation, EKG and blood pressure. In addition, the CAPS system periodically assesses patient alertness by automated response monitoring. With automated response monitoring, patients grip a plastic hand device during the procedure, and are periodically prompted by voice and vibration prompts from the CAPS system to squeeze the device. Longer lag times between the prompt and the squeeze are interpreted as a deeper level of sedation. The initial maintenance rate cannot be more than 75 µg/kg/min, each rate increase cannot be more than 50 µg/kg/min and the overall maximum infusion rate is set at 200 µg/kg/min. To prevent a stacking effect, there is a 180-second lockout period after each infusion rate increase, and a 90-second lockout after each bolus. Finally, hypoventilation, oxygen desaturation or lack of responsiveness will prevent further rate increases, and, if severe enough, can lead the CAPS system to discontinue the propofol infusion. In response to significant hypoxia, the CAPS system will increase supplemental oxygen delivery to the patient and trigger visual and auditory alarms to alert the provider team. To use CAPS, an anesthesia professional must be immediately available in the same building for assistance as needed.
2. Clinical Trial Data
A pilot study involving 48 patients70 was followed by a large, non-blinded multicenter randomized controlled trial,71 in which 1,000 healthy adults undergoing colonoscopy or EGD were randomized to CAPS or MF sedation. The area under the curve for oxygen desaturation (a composite measure of the frequency, severity and duration of hypoxic episodes) was significantly lower for the CAPS group. Furthermore, patient and endoscopist satisfaction were greater for CAPS, and CAPS subjects recovered much faster than the MF controls. The overall incidence of complications was 5.8% for CAPS versus 8.7% for MF. The only serious sedation-related adverse event occurred in a control patient who required transient mask ventilation.
3. Real World Clinical Data
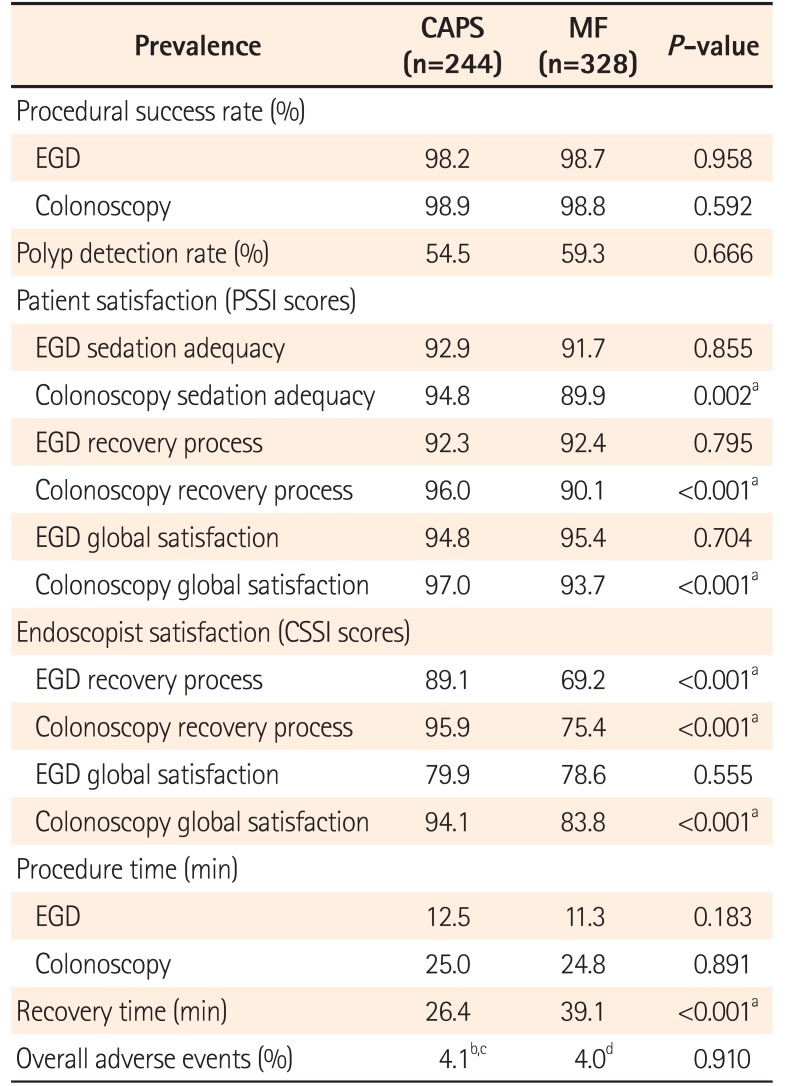
As the only center in the United States to introduce CAPS for large scale, routine clinical use, we assessed the efficacy, safety, efficiency and satisfaction associated with the use of CAPS in a real-world environment. In our first study,72 CAPS was utilized to sedate 55 EGDs and 173 colonoscopy patients; concurrently, 75 EGDs and 223 colonoscopies were performed with MF sedation on controls. Just like in the trials, endoscopists were more satisfied with CAPS than MF sedation. Also, patients were more satisfied with CAPS with regard to recovery parameters (Table 3).7273 Procedural success rates and colonoscopic polyp detection rates were similarly high in both groups. Procedure times were not different, but recovery times were much faster for CAPS than MF. Adverse events were uncommon in both groups. For CAPS, 1 patient required brief mask ventilation, 4 experienced mild hypotension or desaturation, and 5 suffered agitation due to undersedation. For MF, 5 patients had mild hypotension or desaturation, and 8 suffered agitation. There were no instances in which a “code” had to be called or an anesthesia professional had to be summoned to assist with sedation-related complications.

We subsequently reported our 1-year experience with CAPS for colonoscopy on a much larger cohort.74 In this study, 2,677 colonoscopies were performed with CAPS, compared against 2,286 historical MF controls. For CAPS, the procedural completion rate was high (98.8%) and similar to that of controls (99.0%, P=0.526). Polyp detection rates and large polyp detection rates were also similar to that of controls (53.4% vs. 50.1% and 8.2% vs. 8.2% respectively, P>0.01 for both). Mean procedure times were slightly shorter for the CAPS group than the controls (22.2 minutes vs. 22.8 minutes, P<0.001). Again, recovery times were markedly shorter (31.0 minutes vs. 45.6 minutes, P<0.001). In the CAPS group, there were 20 (0.7%) cases of mild oxygen desaturation, 21 (0.8%) cases of asymptomatic hypotension, 4 (0.1%) cases of agitation due to undersedation, and 2 (<0.1%) cases of desaturation requiring transient mask ventilation. In a separate study on a 1-year cohort of 926 patients undergoing EGD with CAPS,75 procedural success rates were again similar to that of MF controls. Procedure times were also similar, but recovery time was markedly shorter. There were 11 (1.2%) cases of mild desaturation, 15 (1.6%) cases of agitation due to undersedation, and 1 (0.1%) case of mild hypotension. In addition, there were 6 (0.6%) patients with desaturation that required transient mask ventilation. Aside from one case of delayed fatality from ischemic colitis believed to be unrelated to sedation, none of the EGD or colonoscopy subjects suffered any severe adverse event such as emergent intubation, hospitalization, permanent injury or death.
Overall, CAPS was found to be a safe, effective and efficient means of providing sedation for EGD and colonoscopy in relatively healthy patients. Even though the rapid recovery associated with propofol does not negate limitations such as the prohibition against driving after the procedure, it has a major impact on patient satisfaction, post-procedural education and endoscopy unit flow.7677 In addition, recovery room staffing was made more efficient, with overtime hours reduced by 32%, resulting in over $14,000 (USD) in savings per month despite increased procedure volumes.78
4. SEDASYS®: Closure and Financial Challenges
At the end of 2016, the manufacturer of SEDASYS® closed down its CAPS division due to the company's inability to project profitability from this technology.79 Between 2014 and 2016, reportedly only 10 or fewer CAPS systems were sold in the United States. Despite excellent safety and effectiveness outcomes, financial factors proved to be decisive in the failure of this product. Currently, there are strong financial incentives to use anesthesia-administered propofol,93563 because anesthesia charges represent a major revenue source for many endoscopy practices in the United States. In many cases, insurance plans will cover anesthesia charges for endoscopy. In fact, Medicare covers anesthesia costs for screening colonoscopies without any deductibles. This policy was intended to increase the uptake of colon cancer screening, despite studies showing that anesthesia use is not associated with any increase in screening rates,80 but will increase costs.81 In situations where insurance coverage for anesthesia is denied, patients are charged directly. These factors limit the number of GI providers willing to invest in a CAPS system, since they would have to absorb the sedation costs. In theory, the endoscopy practice would derive other benefits from CAPS such as decreased recovery times, reduced recovery room staffing needs, and increased patient satisfaction. However, these potential benefits are usually not enough to persuade endoscopy units to invest in the considerable upfront costs of a CAPS system.
NURSE ADMINISTERED PROPOFOL CONTINUOUS INFUSION SEDATION
In our unit, the universal enthusiasm for non-anesthesiologist-administered propofol sedation on the part of nurses, doctors and patients motivated us to develop so-called nurse-administered propofol continuous infusion sedation (NAPCIS), which is a propofol delivery method that replicates the capabilities of CAPS by using programmable intravenous fluid infusion pumps commonly available in the hospital (Alaris® pump module; Becton Dickinson, Franklin Lakes, NJ, USA). Patient selection criteria for NAPCIS are similar to those for CAPS; thus, NAPCIS is reserved for relatively healthy patients undergoing non-advanced, elective, outpatient GI procedures.
1. Mechanics
In NAPS, the propofol is typically delivered as small, frequent intermittent boluses. Given our experience with CAPS, we reasoned that propofol administered as a continuous infusion may be more effective and safer than a bolus strategy,82 even though previous experiences at other centers with continuous infusion propofol had been disappointing.83 NAPCIS delivers propofol as a continuous infusion after an optional loading dose of fentanyl, using a dosing and safety protocol identical to that in CAPS. Towards the end of 2016, we transitioned seamlessly from CAPS to NAPCIS.
2. Preliminary Data
In 2017, we presented preliminary data on NAPCIS.84 Between December 2016 and January 2017, 490 patients underwent outpatient EGD or colonoscopy with NAPCIS at our center. These subjects were compared against 2 historical control groups, consisting of similar low-risk patients who had undergone procedures with CAPS (228) or MF sedation (298). The procedural success rate with NAPCIS was high and similar to that seen in CAPS and MF. NAPCIS procedure times were significantly shorter compared against CAPS and MF; more importantly, recovery times were shorter than CAPS and much shorter than MF (Table 4).84 For NAPCIS, there were 2 cases of transient desaturation that required brief mask ventilation. There were no other serious complications such as intubation, having to call a “code,” unanticipated hospitalization, permanent injury or death. These low complication rates were similar to those seen with CAPS (only one case of mask ventilation) and MF (no mask ventilation). Most endoscopists and nurses found NAPCIS easier to perform than CAPS, and much superior to MF.

We have now performed NAPCIS on over 5,000 patients, with excellent completion rates (>99%), very low complication rates, no serious complications and high patient and endoscopist satisfaction. We believe that NAPCIS is a promising method to deliver non-anesthesiologist administered propofol sedation, but it is important to note that NAPCIS is not designed for medically unstable patients or highly complex endoscopic procedures. Since there is an absolute ceiling for the propofol infusion rate (200 µg/kg/min), NAPCIS may not offer adequate sedation for patients who are very tolerant to sedatives. These more challenging scenarios will still require the expertise of an anesthesia professional delivering general anesthesia or MAC.85
BUNDLED PAYMENTS
Many of the factors that pose as obstacles to the adoption of NAPS and CAPS also apply to NAPCIS as well. These include various regulatory, political and medicolegal issues. However, the most important obstacles are probably financial. At least in the United States, the current insurance coverage system makes MAC more financially attractive than NAPS or NAPCIS for providers,37 thus explaining the dramatic increase in MAC use while the use of non-anesthesia propofol sedation remains uncommon.10 However, with the anticipated advent of bundled payments for screening and surveillance colonoscopy,868788 non-anesthesiologist administered propofol sedation may become more attractive. Colonoscopy is an ideal candidate for bundling because it is a well-defined episode of care with little variability; elective EGD may also be an appropriate candidate. Bundling would involve payment of a prenegotiated amount that would cover the costs of the index procedure, any sedation or anesthesia, any pathologic analysis of biopsies, any repeat procedures (within a short period) performed because of poor bowel preparation or complications such as post-polypectomy bleed, and any secondary examinations such as virtual colonoscopy in cases of incomplete colonoscopy. Other methods of cost control, such as reference pricing, are also being investigated.8990 There is a delicate balance between cost control and maintenance of quality, making this an area of active research.
CONCLUSIONS
In conclusion, endoscopic sedation continues to evolve. In developed countries, it is expected that patients will demand more potent forms of sedation in the future, and thus propofol is likely to assume greater importance. Anesthesia-administered propofol sedation is effective and safe, but is limited by access and cost. CAPS is effective but unfortunately no longer available; nevertheless, non-anesthesia administered propofol sedation continues to be possible in the form of NAPS and NAPCIS. NAPS is already widely used in many European countries. The introduction of bundled payments may eventually make NAPS or NAPCIS the modality of choice in the United States. The roles played by these modalities will be determined by ongoing research on their efficacy and safety, as well by regulatory, medicolegal and financial factors.
Notes
Financial support: None.
Conflict of interest: Otto S. Lin served as a consultant for SEDASYS Inc.