INTRODUCTION
A serrated polyp (SP) in the colon is histologically characterized by a serrated (i.e., saw-toothed) appearance of the crypt epithelium. In the past, most SPs were called hyperplastic polyps (HPs) and were considered to have no malignant potential. However, sessile serrated adenomas (SSAs), which are a subset of SPs, have been recently revealed as a precursor of 20% to 30% of colorectal cancers (CRCs) that are located particularly in the proximal colon.1,2,3 Many studies of adenomatous polyps (APs) have been conducted, and our knowledge regarding SSAs has continued to develop. SSAs are nearly always flat or sessile, may be pale or the same color as the surrounding mucosa, and have vague edges with an adherent mucus layer to obscure the vascular pattern. These are usually >5 mm in size and more often found in the proximal colon.3,4,5,6,7,8,9 Because of their sessile characteristic, SSAs are more difficult to detect and resect endoscopically. This, in concert with their malignant potential and prevalence, makes it more important for SSAs to be identified and managed appropriately.
Many studies have shown that a screening colonoscopy with polypectomy reduces CRC mortality.10,11,12 Despite some minor differences, the current U.S., U.K., and European guidelines on surveillance colonoscopy follow-up after polypectomy are mainly based on the size, number, and histology of polyps.13,14,15,16 Most post-polypectomy surveillance guidelines for SSAs aim to detect early recurrent diseases, such as APs, SSAs, and metachronous CRCs. Recommendations for surveillance colonoscopy follow-up intervals must be based on the characteristics of serrated lesions that are associated with advanced neoplasia, including synchronous and metachronous CRCs. These characteristics include a proximal colon location of the serrated lesions, an increasing number and larger size of serrated lesions, and SSA or traditional serrated adenoma (TSA) histology.2 However, the recommendations lack details regarding the methods, duration, and intensity of surveillance. For example, the British Columbia Medical Association suggests in their post-colorectal polypectomy surveillance recommendations that follow-up colonoscopy should be repeated (1) every 5 years in patients with 1 or more SSAs <1 cm without dysplasia, (2) every 3 years in patients with SSAs >1 cm, SSAs with dysplasia, or (3) within 6 months to verify complete removal in patients with SSAs that were removed without confirmation.17 The Cancer Council Australia suggests in their national bowel cancer-screening program that, at present, there is insufficient evidence to differentiate follow-up protocols for SSAs from follow-up guidelines for standard adenoma.18 The Mayo Clinic suggests in their review article that patients should undergo surveillance every 5 years if they exhibit SSAs <10 mm without dysplasia or every 3 years if their SSAs are >10 mm or exhibit dysplasia.19
The purpose of this study was to determine the proper interval of colonoscopy surveillance aimed at identifying new CRCs in patients diagnosed with SSAs. Hence, we retrospectively analyzed the status and results of follow-up colonoscopy surveillance in South Korea.
METHODS
1. Study Population
We retrospectively reviewed the medical records of patients with SSAs that were diagnosed and removed using colonoscopy and who received 1 or more follow-up colonoscopies at the Digestive Disease Center and Health Promotion Center of Seoul National University Bundang Hospital. The abstracted information included patients' baseline characteristics, such as age, sex, smoking history, education level, and family history of malignancy.
2. Colonoscopy and Pathological Findings
The endoscopic and pathologic characteristics of polyps were reviewed and recorded. Gastroenterologists performed colonoscopies using standard white-light colonoscopies. All polyps were characterized by size, shape, and location. They were removed using cold biopsies or snare polypectomy. Expert gastrointestinal pathologists classified polyps, based on histological criteria, as either an adenomatous (tubular, villous, and tubulovillous) polyp or a SP (HP, TSA, and SSA). SSAs were distinguished from HPs based on the histological criteria. Namely, crypt serrations spanned the entire length of the crypt with complicated lateral spreading or boot-shaped dilated crypt bases in SSAs, but HPs contained crypt serrations in only the luminal halves with narrowed crypt bases. The follow-up interval of surveillance colonoscopy was determined based on the clinical judgment of each colonoscopist.
RESULTS
1. Patients' Baseline Characteristics
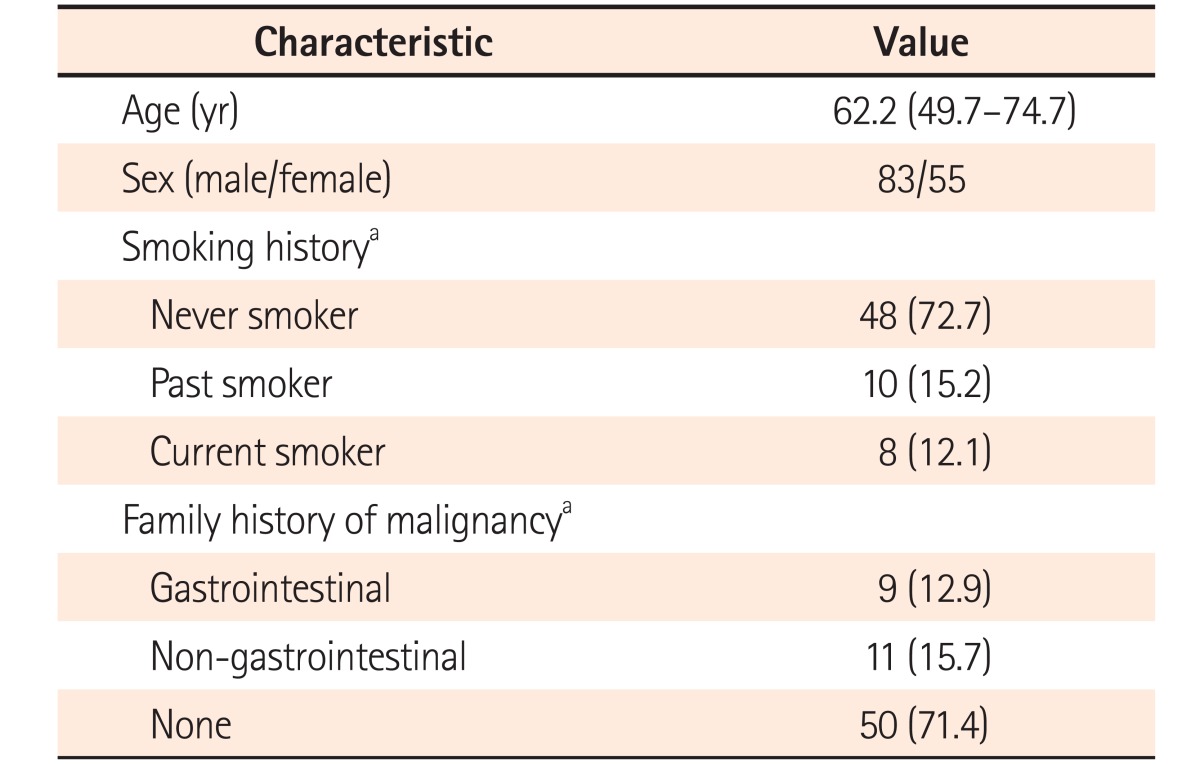
From January 2007 to December 2011, 138 patients were diagnosed with SSAs at the initial colonoscopy. The patients' baseline characteristics are shown in Table 1. The mean age of patients with SSAs was 62.2 years, and 60.1% of patients were men. Most patients underwent colonoscopy at the outpatient department; hence, some data were missing in their medical records.
2. Features of Identified Polyps and Follow-up Colonoscopy Period
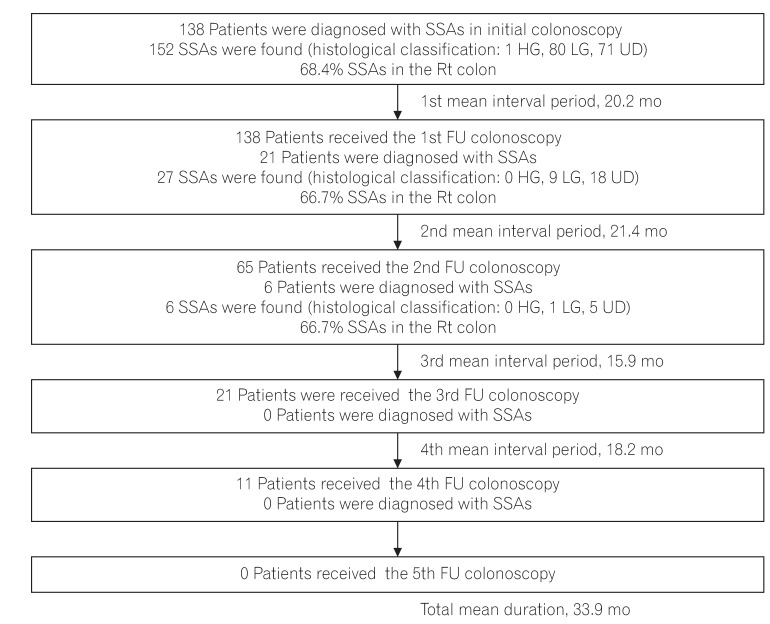
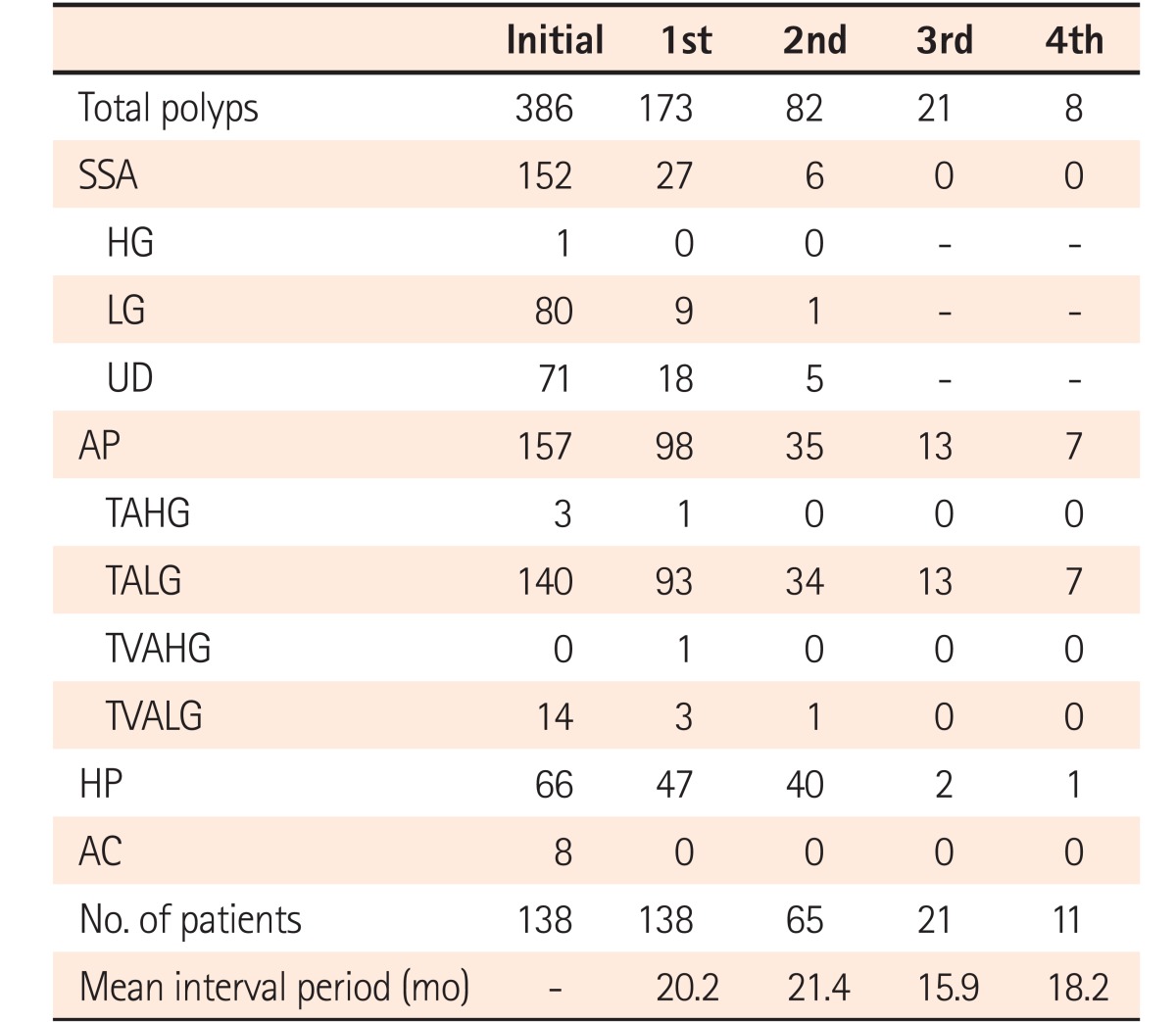
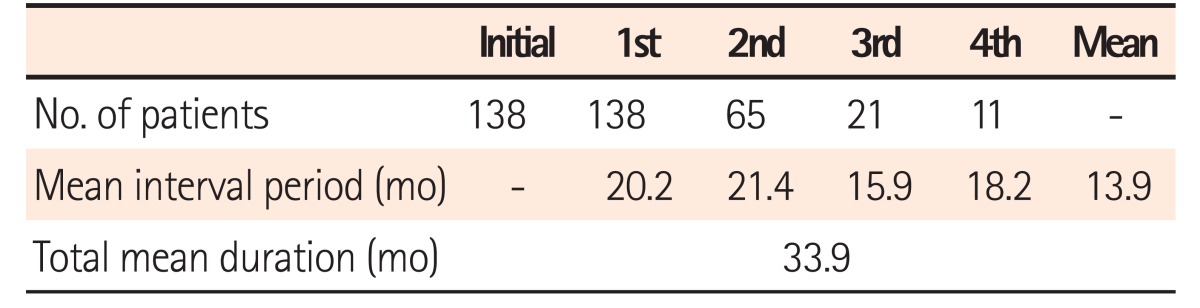
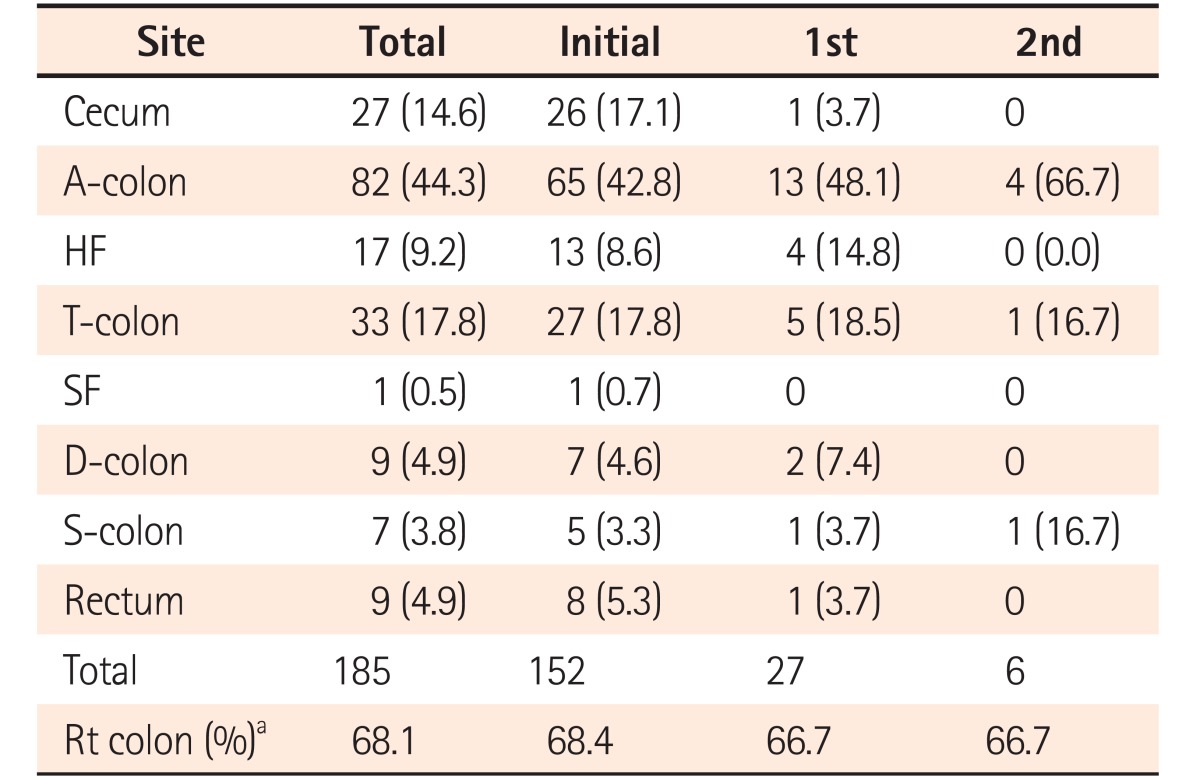
The features of each polyp that was detected and removed at the initial and follow-up colonoscopies are shown in Table 2. At the initial colonoscopy, 386 polyps and 8 synchronous adenocarcinomas were identified in 138 patients. The detection rate of synchronous adenocarcinoma in patients diagnosed with SSAs was 5.8%; however, no metachronous adenocarcinoma was found during subsequent follow-up colonoscopies. At the initial colonoscopy, 152 SSAs were identified in 138 patients, and 68.4% of SSAs were found in the right colon (i.e., from the cecum to the hepatic flexure). The first mean follow-up interval was 20.2 months. At the first follow-up colonoscopy, 27 SSAs were identified in 138 patients, and 66.7% of SSAs were found in the right colon. The second mean follow-up interval was 21.4 months. At the second follow-up colonoscopy, 6 SSAs were identified in 65 patients, and 66.7% of SSAs were found in the right colon. At the 3rd and 4th follow-up colonoscopies, 21 and 11 patients underwent colonoscopy, respectively, and no SSAs were detected. The mean follow-up interval was 15.9 and 18.2 months for the 3rd and 4th colonoscopies, respectively. The total mean duration between the initial and final follow-up colonoscopies was 33.9 months, and the mean interval period between each colonoscopy was 13.9 months. The mean interval period of each subsequent colonoscopy is shown in Table 3. At the fifth follow-up, no patients underwent colonoscopy. The overall schematic of this study is shown in Fig. 1.
3. Site and Size of SSAs Identified at the Initial and Follow-up Colonoscopies
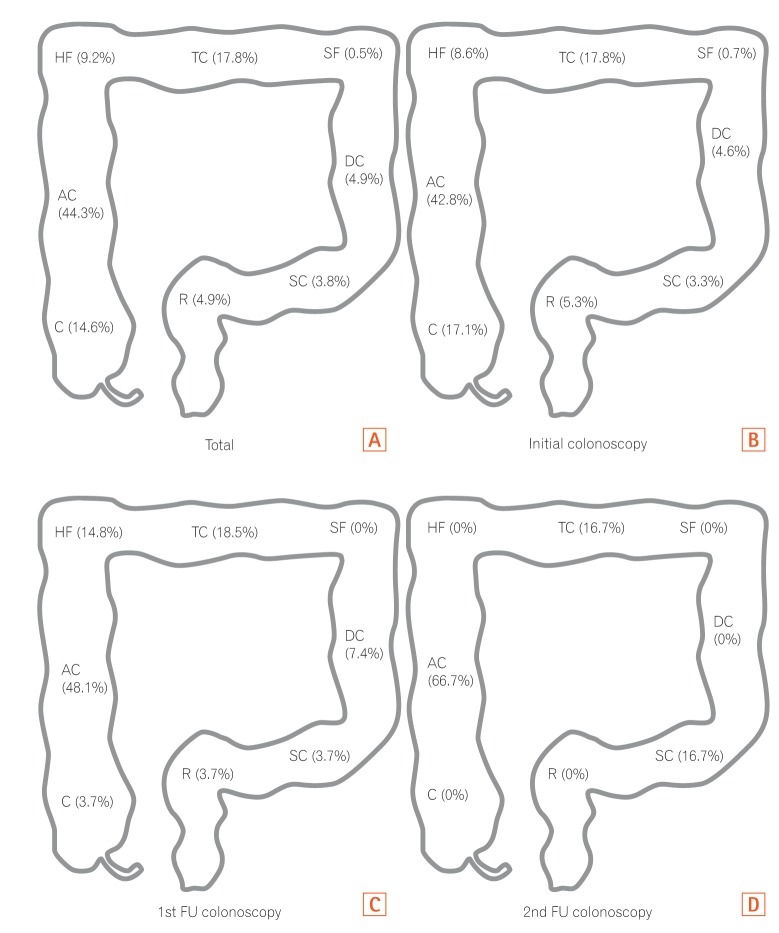
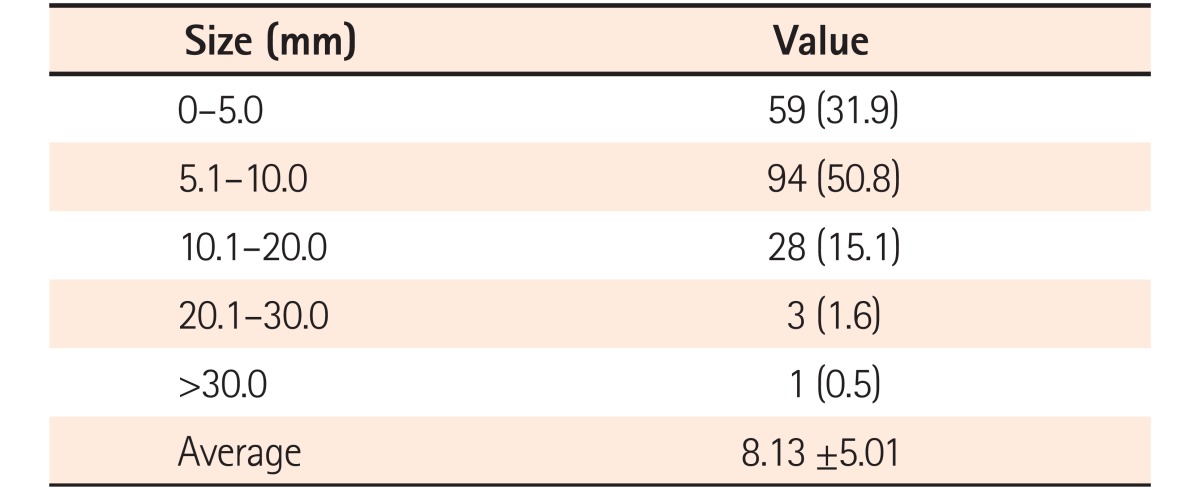
The sites of SSAs identified at the initial and follow-up colonoscopies are shown in Table 4 and Fig. 2. At the initial and follow-up colonoscopies, 68.1% of all SSAs were identified in the right colon, which was the most common site of SSAs identified at the initial and follow-up colonoscopies. The mean size of all SSAs was approximately 8.1 mm (the size distribution of all SSAs is indicated in Table 5). The most common size of SSAs ranged from 5.1 mm to 10 mm. In total, 96 SSAs were removed using snare polypectomy, and 88 SSAs were removed using cold biopsy.
4. Characteristics of SSAs with Synchronous Adenocarcinoma
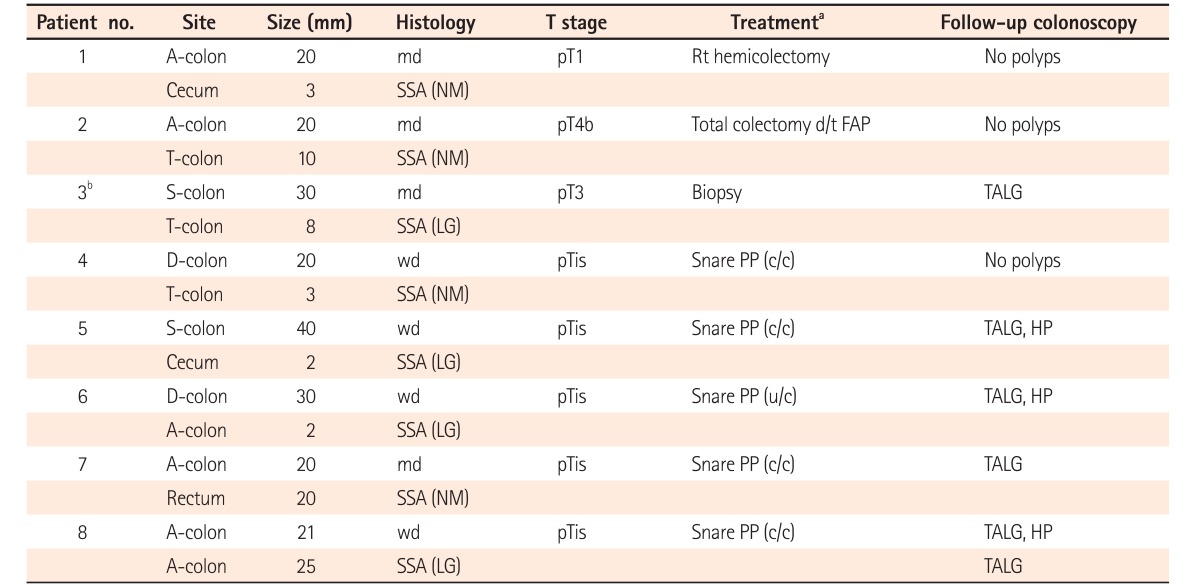
At the initial colonoscopy, we confirmed that the 8 patients diagnosed with SSAs had synchronous adenocarcinomas. Among these 8 synchronous adenocarcinomas, 4 were well differentiated, and the remaining exhibited moderate differentiation histologically. Four were located in the right colon, particularly the ascending colon, and the others were located in the distal colon (descending colon, 2; sigmoid colon, 2). Of the 8 SSAs, 4 showed low-grade dysplasia, whereas the pathological grade was not mentioned for the remaining cases. Four SSAs were in the right colon, and the remaining SSAs were in the distal colon. Two patients with cancer were treated with colectomy, and 5 patients were treated with snare polypectomy. In these cases, the patients were diagnosed with cancer after polypectomy. Only 1 patient with cancer was biopsied at the initial colonoscopy and was treated with chemotherapy because the final diagnosis was sigmoid colon cancer with liver and lung metastases. The characteristics of SSAs and synchronous CRCs are shown in Table 6. The mean size of SSAs with synchronous adenocarcinomas was 9.25Ā±8.75 mm, whereas the mean size of the remaining SSAs was 8.13Ā±5.01 mm. The difference in size was not statistically significant (P=0.550). No CRCs were identified during subsequent follow-up colonoscopy.
DISCUSSION
The most important goal of CRC screening program is the detection and removal of premalignant lesions. Both SSA and TSA have been recently recognized as the precursors of up to 20% of sporadic CRC through the serrated carcinoma pathway.20 Based on a recent report, SSAs comprise approximately 15% of all polyps seen on colonoscopy.21 As shown in recent and previous studies, 4 to 6 large SPs (ā„10 mm) are relatively uncommon (1%-2%). However, proximally located SPs are much more common than large SPs.22,23,24
In this study, 33 SSAs (from 284 detected polyps) were detected using a follow-up colonoscopy, with the detection rate of SSAs being 11.6%. The rate of large SSAs (ā„10 mm) and proximally located SSAs detected using a full colonoscopy is 17.3% and 67.5%, respectively. Such an increased detection rate of SSAs in this study may be due to the increased recognition of the clinical importance of SSAs among gastroenterologists and pathologists.
Many studies on patients diagnosed with sporadic serrated lesions have proved an increased tendency for synchronous and metachronous neoplasia.22,23,24,25,26,27,28 For examples, Hiraoka et al.24 reported that large SPs (ā„10 mm) were related with CRC (OR, 3.34; 95% CI, 2.16-5.03) and that proximal and large SPs were the most important risk factors for proximal CRC (OR, 5.36; 95% CI, 2.40-10.8). Zhu et al.29 reported that colorectal SPs with synchronous CRC, compared with colorectal SPs without synchronous CRC, were related to colorectal SP size ā„10 mm (vs. <10 mm; OR, 4.412; 95% CI, 1.684-11.556; P=0.003) and a diagnosis of SSA or TSA (vs. HP; OR, 6.194; 95% CI, 1.870-20.513; P=0.003 and OR, 6.754; 95% CI, 1.981-23.028; P=0.002, respectively) and SSA and TSA are similarly often associated with synchronous CRC (P=0.460). Therefore, they concluded that histologic subtypes and polyp size may be important markers for synchronous CRC. Leung et al.30 suggested that an important connection was found between synchronous advanced neoplasia and large SPs (P=0.002) or proximal SPs (P=0.013); hence, patients with large or proximal SPs have a higher risk of synchronous advanced neoplasia. However, Ćlvarez et al.28 suggested that large (ā„10 mm) SPs, but not proximal SPs, are associated with the detection of synchronous advanced neoplasia.
In this study, we identified 8 patients with synchronous CRCs, with the proximal colon as the site of SSAs in 50% of patients with synchronous CRC. However, the mean size of SSAs detected with synchronous CRC was 9.25Ā±8.75 mm, whereas the mean size of the remaining SSAs was 8.13Ā±5.01 mm. The difference in size was not statistically significant (t-test, P=0.550). Based on these results, we suggest that proximal SSAs are the more important marker of synchronous CRCs.
Lazarus et al.31 suggested that serrated adenomas are lesions with a significant risk for metachronous serrated adenomas and CRC development. Lu et al.25 suggested that SSAs are high-risk lesions, with 15% of the patients diagnosed with SSA developing subsequent CRCs or APs with high-grade dysplasia and the mean time for the development of CRCs in patients diagnosed with SSA being 8.3 years. Therefore, these facts may not necessarily benefit more frequent surveillance colonoscopy follow-up than is recommended for AP with low-grade dysplasia.
In this study, we did not find any CRCs during a subsequent follow-up colonoscopy, which may be probably because of early endoscopic detection and resection of SSAs/APs as previously reported in the study by Seo et al.32 It may also have been because the number of patients included in this study was small, and the follow-up period was relatively shorter than that in other studies.
This study has several limitations. First, we did not objectively quantify the exact numbers, careers, and the policies on surveillance colonoscopy follow-up interval of each colonoscopist involved in this study because many colonoscopists, including the physicians of the gastrointestinal fellowship training course, have participated in the initial and subsequent follow-up colonoscopies. Second, SSA is often located in the proximal colon, which can lead to differences in detection rates, depending on the status of bowel preparation. Hence, in further studies, the objective value of the degree of bowel preparation should be mentioned. Third, the study was retrospective, and the number of patients enrolled was small, with the ratio of patients lost to follow-up being high. Therefore, a prospective study with larger and longer follow-up periods is necessary to confirm the findings. Further prospective, multicenter, and long-term prospective longitudinal studies are also needed to better understand the natural history of SSA and its association with CRC.
In conclusion, based on our study, we did not find new CRC development in patients diagnosed with SSAs during an annual follow-up colonoscopy. Thus, routine annual follow-up colonoscopy surveillance is not necessary in view of cost-effectiveness to identify new CRC development in all patients diagnosed with SSAs. Instead, we suggest that the proper interval of follow-up colonoscopy for SSAs is determined individually, considering the size and histologic character of each SSA. Furthermore, SSAs occur more frequently in the right colon at the initial and follow-up colonoscopies. Therefore, the right colon should be prepared and examined more carefully.