



Question
A 43-year-old man presented with diarrhea and hematochezia for 1 month prior to hospitalization. He had moderate fever, iron-deficiency anemia, and weight loss of 5 kg in the previous 2 weeks. Physical examination revealed a malnutrition status with a body weight index of 17.5 kg/m2. Neither superficial lymphadenopathy nor hepatosplenomegaly was found.
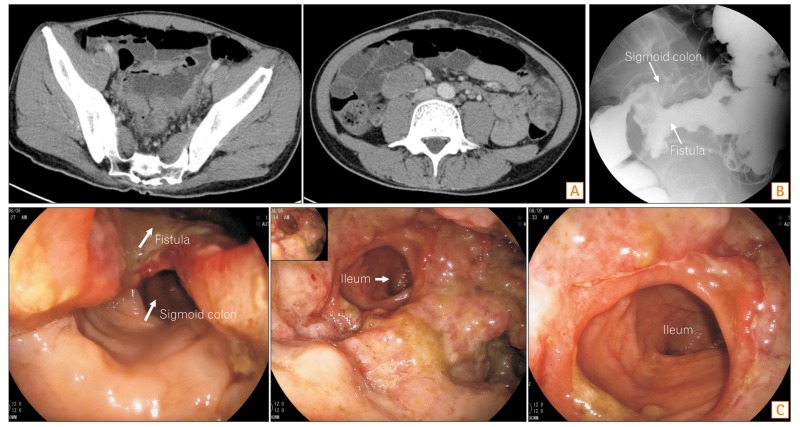
Contrast-enhanced CT of the abdomen revealed the thickened wall of the distal sigmoid colon, an ileosigmoid fistula (Fig. A), and lymphadenopathy in the abdomen and pelvis with a maximum measurement of 4.0×2.6 cm. Barium enema revealed the two paths around the rectosigmoid junction. One was the usual sigmoid colon with remarkable mucosal abnormalities. The other was the ileosigmoid fistula with an irregular lumen (Fig. B). Colonoscopy also clearly revealed a huge ileosigmoid fistula and ulcerative lesions at the rectosigmoid junction (Fig. C). What is your diagnosis of this unusual fistula?
Answer to the Images: Non-Hodgkin's Lymphoma
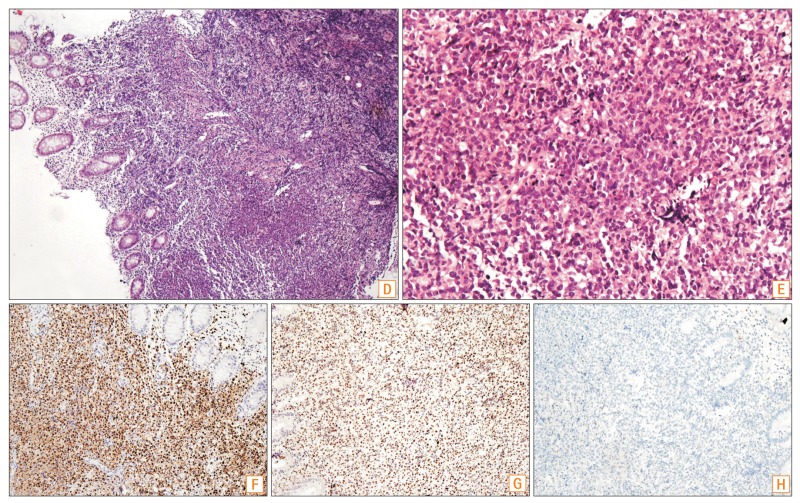
Biopsy specimens were taken from the ulcerative lesions. Pathological examination revealed diffuse infiltration of large lymphoid cells with irregular enlarged nuclei and prominent nucleoli in the mucosa and submucosa (Fig. D, H&E, ×100, and E, H&E, ×400). Immunochemical examination revealed that these atypical cells were strongly positive for CD20 and PAX-5, and negative for CD3 and CD30, and had a high Ki-67 index 80%; which supported the diagnosis of diffuse large B cell lymphoma. Furthermore, the tumor was categorized into the immunochemical subgroup, non-germinal center B type, according to Mum-1 (Fig. F, ×200) and Bcl-6 (Fig. G, ×200) expressions in nuclei and no reaction to CD10 (Fig. H, ×200).
The common causes of internal GI fistulas are CD, diverticulitis, cancer, and iatrogenic injury.1 Primary GI non-Hodgkin's lymphoma involves the stomach (approximately 70%), small bowel (9%), and ileocecal region (7%).2 Intestinal fistula associated with lymphoma is rare. Intestinal perforation can occur spontaneously, act as a surgical complication, or arise from the regressive changes after chemotherapy, which may result in chronic GI fistulas occasionally. Primary GI fistulas that communicate with the guts and various adjacent organs have also been documented, including the bronchus, bladder, spleen, and even aorta.3,4,5
In our patient, chronic ileosigmoid fistula was clearly detected by using CT, barium enema, and colonoscopy. The histopathological examination of the specimens from the ulcerative lesions was critical to the diagnosis of non-Hodgkin's lymphoma. The patient was then transferred to the hematology department to receive chemotherapy.




