Changing epidemiological trends of inflammatory bowel disease in Asia
Article information
Abstract
Inflammatory bowel disease (IBD) has become more common in Asia over the past few decades. The rate of increase in prevalence of the disease varies greatly in Asia, with several countries in East Asia experiencing a more than doubled increase in IBD prevalence over the past decade. Historically, ulcerative colitis (UC) is more common than Crohn's disease (CD) in Asia. However, a reverse trend is beginning to appear in more developed countries in Asia such as Japan, Korea, and Hong Kong. While Asian IBD patients share many similarities with their Western counterparts, there are important differences with significant clinical implications. In Asia, there are more men with CD, more ileo-colonic involvement in CD, less familial aggregation, fewer extra-intestinal manifestations and worse clinical outcomes for older-onset patients with UC. These differences are likely related to the different genetic makeup and environmental exposures in different regions. Evaluation of the differences and rates in epidemiologic trends may help researchers and clinicians estimate disease burden and understand the reasons behind these differences, which may hold the key to unravel the etiology of IBD.
INTRODUCTION
Inflammatory bowel disease (IBD) includes UC and CD. It is a chronic inflammatory disease that involves the gastrointestinal tract and results from a combination of genetic susceptibility, environmental exposure, and dysregulated responses to intestinal microbiota.1 The highest occurrence of IBD is seen in developed countries in North America and Europe, affecting up to 0.5% of the general population.2 Despite its previously low incidence, Asia has been experiencing a significant increase in IBD incidence in the past two decades,34 while Europe has had a plateauing or even decreasing trend of incidence.2 This rapid increase in incidence, coupled to the considerable socioeconomic changes in Asia, has given rise to an opportunity to study the etiology of IBD.
EPIDEMIOLOGY
1. Incidence
The incidences of UC and CD are highest in the West with annual rates as high as 24.3 per 100,000 and 29.3 per 100,000 persons, respectively.25 Despite IBD being much less common in Asia than in the West, it is of concern that the incidence of UC and CD are rising in parallel with rapid urbanization. The highest incidence was mainly reported in East Asia (Korea, Japan, China, Hong Kong) and South Asia (India). A large-scale population-based study of 8 Asian countries (mainland China, Hong Kong, Macau, Singapore, Malaysia, Thailand, Sri Lanka and Indonesia) in 2013 (ACCESS), has shown notable variations in IBD incidence, ranging from 0.54 to 3.44 per 100,000 persons. In this study, the highest annual incidence of IBD was seen in East Asian urbanized areas like Guangzhou (mainland China) at 3.44 per 100,000, with Hong Kong following closely behind at 3.06 per 100,000 and Macau at 2.2 per 100,000 persons. Lower rates were reported in the Southeast Asian countries. There were also notable differences in the incidence of IBD incidence within the same country. In mainland China, the IBD incidence in Guangzhou, Wuhan, Daqing, Chengdu, and Xian were 3.44, 1.96, 1.77, 0.58, and 0.54 per 100,000 persons, respectively.467 These differences have been attributed to the disparate levels of industrialization in these regions or variations in health care systems, including different access to healthcare. Higher UC and CD incidences have been reported in South Korea at 4.60 and 3.20 per 100,000 persons, respectively.
Nevertheless, not all developed countries in Asia share a similar incidence. It is noteworthy that even highly urbanized countries like Singapore and Malaysia have a much lower IBD incidence at 1.06 per 100,000 and 0.94 per 100,000 persons, respectively.4 This may be a consequence of the multi-ethnicity within these countries, with a varying genetic predisposition, lifestyle habits, and other possible unknown environmental factors. To help understand the incidence in different ethnic groups within a country, an analysis of the IBD incidence by race was conducted in Malaysia. The highest rate was seen in Indians (1.91 per 100,000 persons), followed by Chinese (0.63 per 100,000 persons), and Malays (0.35 per 100,000 persons).8 This is also in keeping with a house-to-house survey in Punjab (North India) from 1999 to 2000, which showed a much higher incidence and prevalence rate of UC in the Punjabi populations at 6.02 and 44.3 per 100,000 persons, respectively.9 The distinction in the inter-racial IBD incidence rates supports the likelihood of genetic factors, although different lifestyle and environmental factors may exist for these different ethnic groups. These are important factors to consider when reviewing incidence and prevalence rates in multi-ethnic countries.
Furthermore, rural and urban areas within Asian countries may experience different rates in IBD increases. One such example is a recent hospital-based study in Korea from an area outside of the city of Seoul, which demonstrated lower rates of complicated disease. Long-term population-based epidemiological studies covering rural as well as urban areas within Asia would help us understand the characteristics of IBD in this region and the interregional differences.10
2. Prevalence
IBD is a chronic disease that involves young patients. In addition, its rapidly increasing incidence together with the better access and delivery of healthcare is resulting in an exponential growth in the prevalence of IBD in Asia. The effect of compounding prevalence11 of IBD in Asia is crucial for future healthcare planning, as existing systems in newly industrialized countries may not be ready for the staggering increase in disease burden. From 1991 to 2005, the prevalence of UC in Japan has increased by 3.5-fold from 18.1 to 63.6 per 100,000 persons, while the prevalence of CD has increased by 3-fold from 5.9 to 21.1 per 100,000 persons.1213 The latest information available from the Japanese National IBD registry has shown that the prevalence of UC and CD has increased significantly to 121.9 and 30.1 per 100,000 persons respectively in 2013.14 This observation emphasizes the importance for healthcare systems in Asia to pre-emptively invest resources in preparation for the burgeoning IBD burden.
3. Temporal Trend
In general, UC tends to appear first in areas with emerging IBD, followed by CD at a variable interval. In North America, the incidence of UC and CD increased from 8.3 and 6.9 per 100,000 persons, respectively, in 1993,15 to 14.3 and 14.6 per 100,000, respectively, in 2004.16 A similar trend was also observed amongst Asian countries in the past few decades. Incidences for both UC and CD were rapidly rising in Asia, with CD having a steeper increment in more developed countries, resulting in a reducing UC:CD ratio over time. A large prospective population-based epidemiological study from South Korea (Korean Association for the Study of Intestinal Diseases [KASID]) showed at least a 10-fold increase in the incidence of UC and CD over two decades. The UC and CD incidence rates increased from 0.34 and 0.05 per 100,000 persons, respectively, from 1986 to 1990, to 3.08 and 1.34 per 100,000 persons from 2001 to 2005. There is also a reduction in the UC to CD ratio from 6.8 to 2.3 during the same period, demonstrating a sharper rise in CD incidence over time.17 More recent Korean data have reported that the incidence of UC and CD have further increased to 5.0 and 3.6 per 100,000 persons, respectively, in 2006. Within this same study, both the incidence of UC and CD were observed to have stabilized and perhaps are showing a slight reduction trend; the most recent incidence for UC and CD in 2012 was 4.2 and 3.1 per 100,000 persons, respectively.18
Table 1 summarises the available incidence and prevalence rates of IBD in various Asian countries.
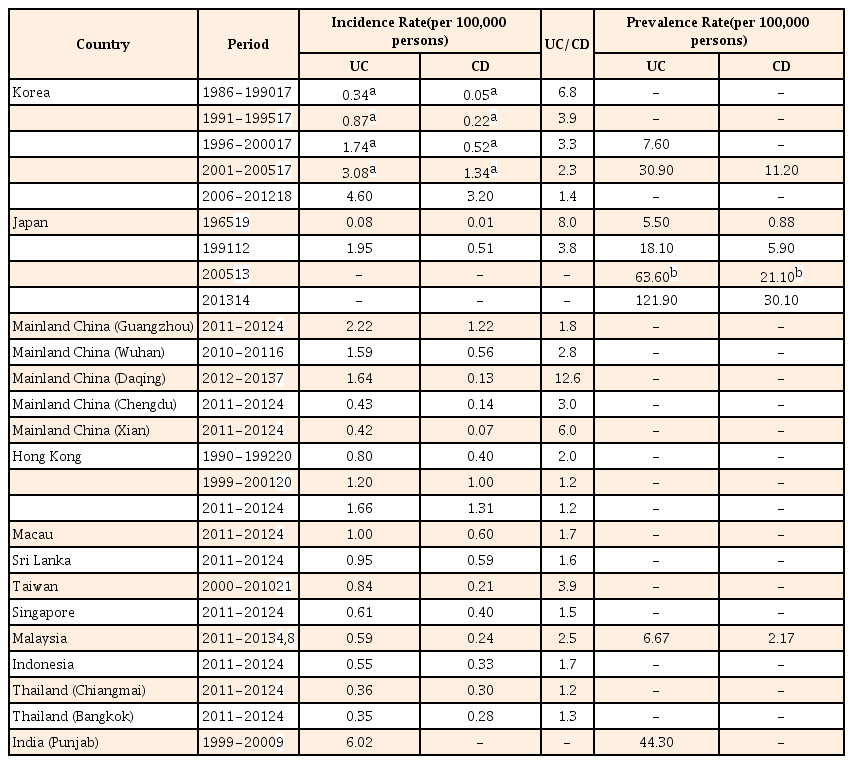
Incidence and Prevalence Rates of IBD in Various Asian Countries
GENETIC FACTORS
There is varying genetic predisposition to IBD in different regions. Major nucleotide oligomerisation domain (NOD2) variants in Caucasians have not been identified in many of the Asian ethnicities (Han Chinese, Japanese, Korean, Indian and Malaysians).22 However, novel NOD2 mutations associated with CD have been reported in Malaysians (JW1 mutation) and Han Chinese and Indians (P268S mutation).23 Amongst Asian populations, tumor necrosis factor superfamily 15 (TNFSF15) polymorphisms are associated with CD, while the TNF α-308 polymorphism is associated with UC. A recent large-scale trans-ethnic study has also demonstrated the significant genetic heterogeneity between East Asian, Indian, and Iranian populations in Asia.24 Identification of novel genes and genetic variants in Asian patients will help us comprehend the genotype to phenotype contribution to IBD's disease course and also explain the differing genetic predisposition between ethnicities.
While genetic factors are important in the pathogenesis of IBD, genetic predilection alone is insufficient to result in disease manifestation. Studies of monozygotic twins report a concordance rate for CD ranging from 20% to 50% and a much lower rate for UC,252627 advocating for the presence of other important environmental factors in the development of IBD.
ENVIRONMENTAL FACTORS
Environmental factors play an integral role in IBD pathogenesis. A prospective study evaluating South Asian immigrants to Leicester, United Kingdom (UK), has shown that UK born children of South Asian descent had a comparable risk of developing UC as the local population,28 despite having lower rates of UC in their native countries. Such studies have been pivotal in substantiating the role of environmental factors in the development of IBD.2930 A more recent retrospective study of a population-based cohort of IBD patients in Ontario, Canada, has reported the association of younger age of immigration to Canada and an increased risk of IBD (14% increased risk per younger decade of life at immigration). Canadian-born children of immigrants from some regions (Middle East/North Africa, South Asia, Sub-Saharan Africa) assumed an equally high IBD incidence as children of non-immigrants, supporting the importance of early-life environmental exposures in the development of IBD.3132
1. Smoking
Western studies reported smoking as a consistent factor associated with IBD, increasing the risk of CD but reducing the risk of UC.33343536 Furthermore, actively smoking CD patients undergo a worse disease trajectory, with a higher risk of relapse after remission. On the contrary, UC patients are more likely to have a disease flare after smoking cessation.37 It appears that smoking does not have such a marked impact on Asian CD patients. At a population level, Western countries like Canada and Sweden with a high CD incidence have a lower prevalence of smoking in the adult population (<30%). In comparison to Asian countries with a much higher smoking prevalence (>65% of men), a much lower CD incidence has been reported. This observation suggests that although smoking is an important risk factor for CD, it could only influence the disease course but may not be sufficient to affect population trends in IBD.38
2. Appendectomy
Asian studies from Japan39 and China40 have shown that appendectomy is associated with a decreased risk of developing UC, similar to the Western data.41 The notion of appendicitis rather than appendectomy having a protective effect against UC in the Western population,4243 does not have any corroborative data in Asia. Currently, there is no convincing evidence to associate appendectomy to the development of CD.
3. Diet
Several studies from the West have reported that increased consumption of linoleic acid44 and animal protein45 are associated with an increased risk of IBD, especially for UC in healthy women. Increased intake of fats, fatty acids, sugar, and meat are correlated with an increased risk of UC relapse.46 High sugar consumption has also been reported to increase the predisposition to develop CD.47 On the contrary, increased fiber, fruit, and vegetable intake seem to reduce the risk of IBD development.48 Studies from Japan have reported similar findings, showing that increased intake of sweets, fats, fatty acids, meat, and oil correlate with the increased risk of developing IBD.4950 A recent case control population-based study involving 9 different Asia Pacific countries (ACCESS) has reported that more than 12 months of breast feeding has a marked protective effect on the development of both UC and CD. Consumption of tea or coffee has also been noted to have a protective effect51 against IBD.
4. Antibiotics Usage
Several observational studies from the West have shown an association between antibiotic usage and the subsequent diagnosis of IBD, although the causality has not been proven.525354 In contrast, the only available Asian study has reported a protective effect of childhood antibiotics against the development of UC and CD. This paradoxical effect might be a consequence of childhood antibiotics usage being a surrogate for gastrointestinal infections, which in turn result in the induction of tolerance.51
CLINICAL PRESENTATION
Many of the clinical manifestations of IBD in Asia share similar characteristics to patients in the West. Nonetheless, there are several notable differences that are relevant to physicians.
1. Sex
There seems to be an overall female preponderance for IBD in the Western literature.5556 In Canada, the women to men incidence rate ratio can be as high as 1.53 for CD and 1.21 for UC in certain provinces.55 However, what is more consistently observed is the female preponderance for CD but an equal or slight female preponderance in UC. On the contrary, Asian data seem to support a male preponderance for CD, but an equal or slight male preponderance for UC. The men to women ratio in Asia for CD was as high as 2.83.1720215758 Thus far, there has not been a proven cause for such a phenomenon. Possibilities would include a different genetic susceptibility and men having greater chances to seek education or job opportunities in industrialized areas at a younger age, which increases their early-life exposure to potential environmental risk factors. Continued monitoring of the epidemiological evolution in Asia will be important to detect any reversal of the sex ratio over time, to parallel that of Western data.
2. Age
Multiple Western studies have reported a bimodal distribution in the age at diagnosis of IBD patients, with a younger peak age at 20 to 30 years for CD, 30 to 40 years for UC, and a lower second older peak at 60 to 70 years for both diseases.59 This bimodal distribution by age has not been consistently reported in Asia, with several newer Asian studies demonstrating only the presence of a first peak at a comparable younger age and a much less prominent second peak.917206061
3. Disease Presentation and Course
Clinical presentations for UC are comparable between Asian and Western populations, with some Chinese data reporting a milder disease course and less fulminant colitis.6061 More differences are noted between Asian CD patients and their Western counterparts. Ileal, colonic, and ileocolonic involvement are usually found in equal proportions in the Western CD population. Data from East Asia has observed that ileocolonic disease is the most common CD phenotype, with 71.0% in Guangdong (China),62 66.7% in South Korea,17 65.8% in Japan,63 and 50.5% in Hong Kong.64 More heterogeneity in CD disease involvement is noted in South and West Asia.6165 Of significance, perianal disease is commonly detected in East Asian patients, involving 58.8% of CD patients in Guangdong (China),62 43.1% in Korea,66 and 30.3% in Hong Kong.64 This is higher than the Caucasian CD data, with reported rates in CD patients with perianal disease up to 29.6% in a multi-center American and European study,67 26.6% in New Zealand,68 and 25.1% in France.69 It has also been reported that colectomy rates for UC and CD are lower in Asia (1% at 1 year), with the exact reason yet to be determined. Postulations included a milder UC course and a higher threshold to perform colectomy in Asia.6570
4. Family History
Familial aggregation among IBD patients is commonly reported in the Western population, and is more frequently noted in CD than UC.71727374 A systematic review has noted that 0% to 3.4% of Asian IBD patients have familial aggregation, which is much lower than the reported rates of 10% to 25% in Western countries.75
5. Extra-intestinal Manifestations (EIM)
There is a significant variation in the prevalence of EIM in Asia, with the highest reported prevalence in India, involving around one-third of the IBD patients.7576 In contrast, the reported prevalence of EIM in East Asia is significantly lower at 6% to 14%,65 compared to 21% to 41% in the West.777879
6. Colorectal Cancer (CRC)
Available Asian data indicates a lower overall prevalence rate of 2.2% of UC related CRC406480818283 compared to the 3% to 5% in the West.8485 However, it is important to note that the available Asian studies have shorter durations of follow-up. Other contributory factors for lower reported CRC rates in Asia include the shorter UC history in the region and also relatively lower disease prevalence. It is probable that the prevalence of UC-related CRC will increase in parallel with the increasing disease prevalence and duration of disease in Asia.
7. Older-onset IBD
Older-onset IBD refers to patients diagnosed with IBD at an age above 60 years. Studies from Western countries have generally reported a less aggressive course of IBD,86 especially for UC.868788 In contrast, Asian older-onset UC patients tend to have a similar,89 if not worse, outcome than the younger-onset UC patients.9091 A Hong Kong retrospective population-based study has reported that older-onset UC is associated with a higher risk of suffering from opportunistic infections like cytomegalovirus and Clostridium difficile , higher rates of hospitalization for UC flares, CRC, all-cause mortality, and UC-related mortality compared to younger-onset patients.90 This disparate clinical course is clinically important, because it accentuates that the available Western data do not necessarily translate to similar trends in Asia. This finding advocates for ongoing Asian IBD epidemiological studies to detect such dissimilarities.
A recent systematic review and meta-analysis of available studies worldwide has observed that older-onset CD patients are more likely to have isolated colonic involvement, which are predominantly inflammatory in nature and are infrequently associated with perianal disease. Older-onset UC is more similar to younger-onset UC, with a slightly higher likelihood of left sided colitis but not pancolitis. Although immunomodulators and biologics are less commonly used in older-onset IBD patients, this was not supported by lower surgical rates. On the contrary, older-onset UC patients have higher rates of surgery, suggesting that the disease course for olderonset IBD is not more benign than younger-onset disease.92
CONCLUSIONS
An exponential increase in the prevalence of IBD within Asia is of concern and it is imperative that Asian healthcare systems are prepared for this. Despite this being the same condition afflicting both Western and Asian populations, there are several significant variations in its phenotype, possibly as a result of the differences in genetic composition and environmental influences. Physicians should be cognizant of these differences and be prepared to individualize management for their patients. Evaluating the differences between Asian and Western IBD data will help us better understand the etiology of IBD. Well-conducted epidemiological studies in more areas with different rates of urbanization within Asia are essential for us to achieve this goal.
Notes
Financial support: Dr. Sunny H. Wong is supported by the Croucher Foundation, Hong Kong.
Conflict of interest: None.
