INTRODUCTION
Although the cause of IBD is not clear, recent progress in the analysis of intestinal microflora suggests that changes in the intestinal microflora are associated with IBD onset and exacerbation [1]. Many exogenous microorganisms, such as Clostridium difficile and cytomegalovirus potentially induce acute and/or chronic intestinal inflammation, which can alter the intestinal microflora and affect the clinical course of IBD [2-4].
Helicobacter pylori, a Gram-negative, spiral-shaped, microaerophilic bacterium that colonizes the gastric mucosa of humans and non-human primates, is a major cause of exogenous infection, and is closely associated with atrophic gastritis [5], gastroduodenal ulcers [6], gastric cancer [7,8], mucosa- associated lymphatic tissue lymphoma [9], and idiopathic thrombocytopenic purpura [10]. H. pylori eradication therapy to treat or prevent these diseases is generally performed by administering triple therapy with a proton pump inhibitor, amoxicillin, and clarithromycin or metronidazole for 7 days, with eradication rates ranging from 80% to 90% [8,11,12]. Although 10% to 30% of patients experience some complications such as diarrhea and loose stool, the benefits of eradication regimens are fully acknowledged for patients without complicated diseases [13]. H. pylori infection and its eradication can alter gastric microflora [14], but analyses of the intestinal microflora have not been reported, except for one study of eradicated patients with an altered microbiome in which Bacteroides was decreased and Firmicutes was increased [15]. The incidence of concomitant H. pylori infection is lower in IBD patients than in a non-IBD cohort [16], suggesting that H. pylori infection protects against IBD and thus eradication therapy could be harmful for IBD by altering the gastric acid content and changing the intestinal microbiota. In contrast, the efficacy of 3 kinds of antibiotics (amoxicillin, tetracycline, and metronidazole) for 2 weeks was reported for patients with UC [17], suggesting that H. pylori eradication therapy can be safely performed for UC patients without inducing disease exacerbation, but direct evidence of the effect of H. pylori eradication on the disease course of IBD patients has not been reported. In addition, the H. pylori eradication rate for IBD patients has not yet been reported. We performed a multicenter, retrospective cohort study to elucidate the safety and efficacy of H. pylori eradication therapy for IBD patients.
METHODS
1. Ethical Considerations
The overall study meets the intent and requirements of the Declaration of Helsinki, Ethical Guidelines for Medical and Health Research Involving Human Subjects by the Ministry of Health, Labour, and Welfare-Japan and by the Japanese Ministry of Education, Culture, Sports, Science and Technology-Japan. The institutional ethics committees of each participating institution approved this study.
2. Patients
This was a multicenter, retrospective cohort study conducted at 25 institutions in Japan. Outpatients with IBD (UC or CD) who underwent eradication therapy for H. pylori with acid-suppressive drugs and amoxicillin-based triple-therapy from March 2005 to July 2015 were included (eradication group). After searching patients by prescription history and/or International Classification of Diseases (ICD)-10 codes, basically all eradicated IBD patients were enrolled except ones whose detailed medical records during eradication could not be obtained. To establish a non-eradication control group (non-eradication group), 2 paired IBD patients without H. pylori eradication in the same institution were included by selecting the next 2 consecutive outpatients after the date of prescribing eradication drugs for each eradicated patient, and matching them by sex, age (within 10 years), and disease location and severity. We did not have any standard values to establish the number of enrolled patients. The infection rate of H. pylori in all Japanese population is around 20% in their 50’s [18], and the rate in IBD patients was reported to be almost half of that in non-IBD cohort [16]. And we hypothesized that the detailed clinical courses after eradication therapy could be obtained in 20% of IBD patients for whom H. pylori infection was checked. Overall, we estimated that 2% (100 patients) in 5,000 IBD patients in participating institutions could be enrolled as eradication group. And we used 1:2 design to enhance the reliability of the present study as much as possible. Prior to the patient enrollment, we had set the above study design and the ethics committee approved the design. Patient inclusion was decided by the IBD specialists or gastroenterologists at each institution, and the patients were given the right to opt out the study.
3. Medical Records
Baseline clinical information for all patients was obtained, including sex, age, BMI, disease duration and location, blood type, smoking and drinking status, history of abdominal surgery for IBD, medications, and disease activity. In the eradication group, detailed information of the H. pylori eradication was obtained, such as the modality of diagnosing H. pylori infection and eradication, indications for eradication therapy, number of eradication treatments, eradication regimen, and success of eradication. The H. pylori status of the non-eradication group was also determined. In both groups, disease activity of IBD at baseline, and at 2 and 6 months after eradication/observation was obtained, and severe adverse events were collected. The survey forms were retrospectively collected and submitted from the participating institutions to the Department of Gastroenterology and Hepatology, Osaka University Graduate School of Medicine.
4. Definition of Disease Exacerbation
To ensure maximum objectivity and measurability for assessing disease exacerbation in this retrospective study design, we obtained information for all participants regarding “increase or addition of IBD drug,” “IBD-associated hospitalization,” and “IBD-associated surgery” after 2 and 6 months of eradication/observation, and cases meeting any of the above conditions were defined as IBD exacerbation. The physician’s global assessment was applied to all participants for analysis of disease exacerbation and improvement. Disease activity indices such as the clinical activity index (CAI) for UC [19,20] and the CDAI for CD [21] were also obtained, and higher and lower scores from a baseline CAI score of ≥3 and a baseline CDAI score of ≥70 were considered disease exacerbation or improvement, respectively.
5. Endpoints
Prior to the approval of the ethics committee and subsequent patient enrollment, we established the primary endpoint of the study as the difference in the IBD exacerbation rate (defined) after 2 months of observation between the eradication group and the non-eradication group. Secondary endpoints were the difference in the exacerbation rate at 6 months of observation, the physicians’ global assessment, and disease activity indices between groups. In the eradication group, the eradication success rate, difference in IBD exacerbation between eradication success and failure, and adverse events after eradication were also set as secondary endpoints.
6. Statistical Analysis
Statistical analyses were performed using Pearson chisquare test, and univariate and multivariate logistic regression analyses were performed with factors associated with disease exacerbation. All data obtained from the study were analyzed using JMP Pro version 12.1.0 (SAS Institute Inc, Cary, NC, USA) and a P-value of less than 0.05 was considered statistically significant.
RESULTS
1. Characteristics of the Participants
A total of 437 IBD patients were enrolled in this study. Eight patients were excluded due to incomplete data, and thus 429 participants were included in the analysis (Supplementary Fig. 1). Participants comprised 144 patients in whom H. pylori was eradicated (eradication group) and 285 control patients (non-eradication group); 88.1% of the patients had UC and the others had CD. One hundred thirty-eight patients (32.2%) had limited disease (proctitis in UC [E1] and terminal ileitis in CD [L1] in Montreal classification [22]), and 380 patients (88.6%) were in remission at baseline. There were no significant differences in the baseline clinical parameters between the eradication group and non-eradication group, except for the lower use of 5-aminosalicylic acid in the eradication group (P= 0.012). Detailed characteristics are provided in Table 1.
2. Disease Activity after H. pylori Eradication
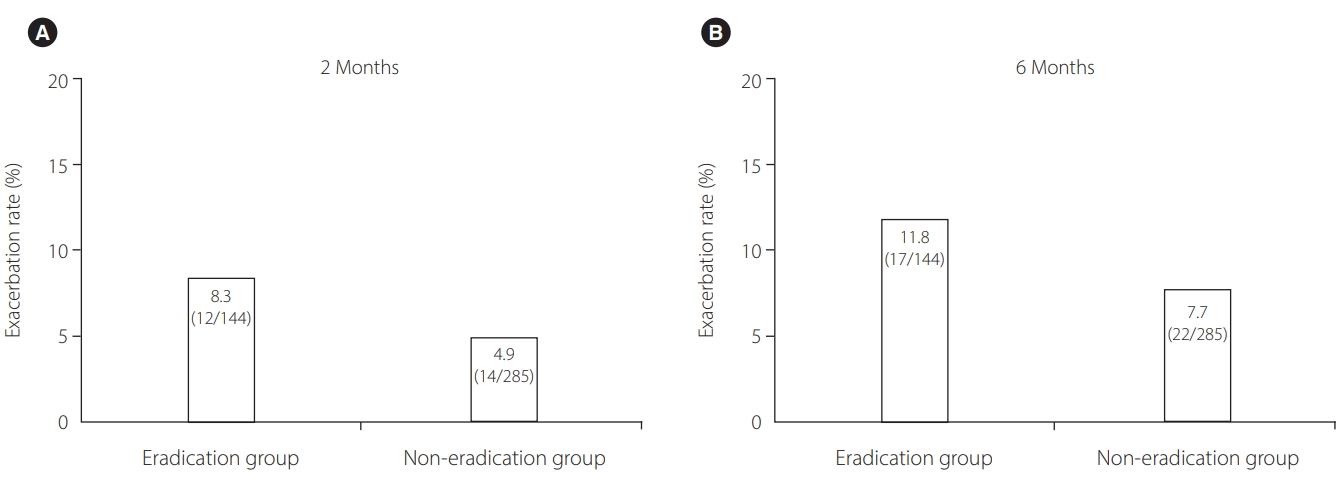
We first analyzed the primary endpoint of the study by comparing the rate of IBD exacerbation between the eradication group and non-eradication group at 2 months. The IBD exacerbation rate in the eradication group was 8.3%, and did not differ significantly from that in the non-eradication group (4.9%; OR, 1.76; 95% CI, 0.78-3.92, P= 0.170) (Fig. 1). The IBD exacerbation rate at 6 months was also not significantly different between groups: 11.8% in the eradication group and 7.7% in the non-eradication group (OR, 1.60; 95% CI, 0.81-3.11; P=0.172) (Fig. 1). We also investigated the IBD exacerbation rates in UC and CD. In both diseases, the differences were also not observed between 2 groups (Supplementary Table 1). Next, changes in disease activity following H. pylori eradication were analyzed by the physicians’ global assessment. Analysis of patient outcomes according to 3 categories (exacerbated, unchanged, and improved disease) at 2 months revealed that none of the patients in the eradication group had improved whereas 3.2% (9/285) of patients in the non-eradication group had improved, and the difference between groups was significant (P=0.019) (Table 2). Moreover, changes in the disease activity indices were investigated. Analysis of 82.7% (350/423) of patients analyzed at 2 months and 81.1% (343/423) of patients analyzed at 6 months revealed no significant differences in disease activity between groups (Supplementary Table 2). Together, these results indicate that H. pylori eradication therapy does not exacerbate IBD or improve disease activity.
3. Factors Associated with IBD Exacerbation after H. pylori Eradication
We next investigated the factors associated with disease exacerbation by H. pylori eradication. Univariate analysis including all participants indicated that female and active disease at baseline tended to be risk factors of definition-based exacerbation at 2 months (Table 3). We then performed a multivariate analysis using a logistic regression model for these 2 categories above, as well as H. pylori eradication, which identified active disease an independent factor of exacerbation (OR, 3.57; 95% CI, 1.37-8.61; P=0.011). We also analyzed the factors of exacerbation in only the eradication group. Univariate analysis was performed by additionally including eradication-associated factors, such as frequency of eradication treatment, eradication regimen, and success of eradication. The analysis identified use of corticosteroids as a significant risk for exacerbation, and biologic agents and active disease tended to be risks for exacerbation (Table 4). Although multivariate analysis was not performed because of the small number of exacerbated patients, these findings suggest that active disease, but not H. pylori eradication, is an independent risk for disease exacerbation, and that use of corticosteroids can be associated with disease exacerbation after H. pylori eradication.
4. Disease Course after IBD Exacerbation
Next, the detailed disease courses of exacerbated patients were investigated. In 12 patients experiencing disease exacerbation within 2 months in the eradication group, exacerbation occurred 33±21 days after H. pylori eradication, but the exacerbation was mild in all patients and 11 patients recovered while 1 remained unchanged by medical therapy. At the 6-month observation in all patients, the rates of overall IBD-related hospitalization, IBD-related surgery, and severe adverse events other than IBD exacerbation were 1.4% (6/421), 0.5% (2/421), and 0.2% (1/421), respectively, with no significant differences between the eradication group and non-eradication group.
5. H. pylori Eradication Regimen and IBD Exacerbation
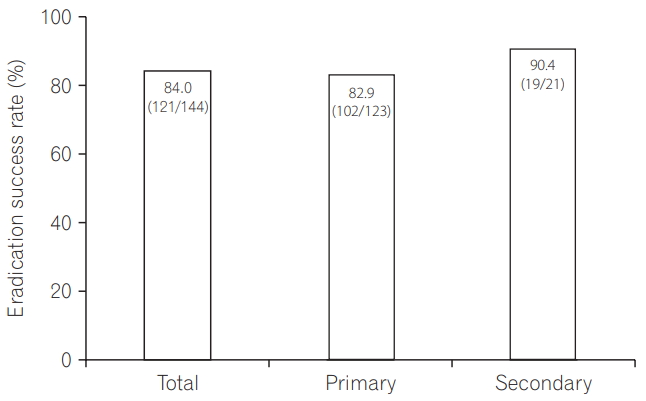
Finally, H. pylori status and H. pylori eradication success rates were investigated in the eradication group. Characteristics at H. pylori eradication are shown in Supplementary Table 3. Overall eradication success rate was 84.0% (121/144). Among 144 eradicated patients, 123 patients (85.4%) received primary eradication therapy, and the eradication success rates of primary and secondary therapy were 82.9% (102/123) and 90.4% (19/21), respectively (Fig. 2). Differences in the acid-suppressive drugs used at eradication were not associated with exacerbation of IBD (Table 5). We also investigated the exacerbation rates in clarithromycin and metronidazole. Disease exacerbation rates in 2 months were 9.2% (11/120) in clarithromycin group and 4.6% (1/22) in metronidazole group, and differences were not significant (OR, 2.12; 95% CI, 0.26-17.3; P= 0.474). The rates in 6 months were 11.7% (14/120) in clarithromycin group and 13.6% (3/22) in metronidazole group, with no significance between 2 groups (OR, 0.84; 95% CI, 0.22-3.22; P=0.794). These data indicate that eradication regimen was not associated with IBD exacerbation at least amoxicillin-based triple therapy during 6 months period.
DISCUSSION
Here, we report the results from a multicenter retrospective cohort on the disease activity of IBD patients who underwent H. pylori eradication therapy. Our data clearly demonstrated that H. pylori eradication did not exacerbate IBD and induced no severe adverse events. On the other hand, we revealed that H. pylori eradication therapy did not improve IBD. Moreover, the eradication success rate was comparable to that in previous reports in which eradication therapy was performed for patients without IBD [23]. Although the influence of eradication therapy was prospectively observed in only 6 CD patients and unchanged disease activity was reported [24], this was small study without control arm and no UC patients were included. Our present report clearly described the disease activity of both CD and UC patients after H. pylori eradication in larger cohort with control arm.
The prevalence of concomitant H. pylori infection is low in IBD patients compared with non-IBD populations [16,25], suggesting that H. pylori infection itself might be protective against IBD. H. pylori infection mainly occurs in early childhood in countries with a high-prevalence [26], and IBD can generally develop after H. pylori has colonized in the stomach. In the present study, H. pylori eradication did not affect the disease activity of IBD, suggesting that the association between IBD and H. pylori infection may be weak at least in short-term disease course. Additional study is needed to clarify whether long-time H. pylori infection can affect disease course of IBD.
Eradication of H. pylori using acid-suppressive drugs and antibiotics can alter intestinal microflora [27,28], which could potentially affect the disease activity in IBD patients with reduced microbial diversity [29]. In addition to the report that triple antibiotic combination therapy using amoxicillin, tetracycline, and metronidazole for 2 weeks improves UC [17], a systematic review of studies of adult patients receiving any dose of antibiotic therapy for at least 7 days and up to 16 weeks for active disease also demonstrated a statistically significant benefit of antibiotic treatment for inducing remission in patients with active UC [30]. In the present study, however, we did not observe a better outcome of IBD following H. pylori eradication therapy. A 1-week treatment with 2 types of antibiotics may not provide enough of a therapeutic effect, such as reducing relapse, for quiescent IBD patients. The safety of antibiotic treatment for patients with quiescent UC, which comprised 90% of patients in the present study, has not been reported. Further analysis is needed to evaluate the safety of antibiotic therapy for patients with quiescent UC.
Although the number of CD patients enrolled in the present study was small, there were no differences in the disease course after eradication therapy between CD and UC patients (Tables 3, 4 and Supplementary Table 1). Moreover, additional detailed investigation of patients whose disease exacerbated within 2 months after eradication revealed no severe adverse events, and almost all cases recovered with appropriate treatment. These results indicate that H. pylori eradication therapy is generally feasible even for IBD patients. Moreover, the multivariate analysis indicated that high disease activity, but not H. pylori eradication, was an independent factor for IBD exacerbation (Table 3). Analysis for the only eradicated patients also showed that use of corticosteroids was significantly associated with disease exacerbation after H. pylori eradication (Table 4). Although the direct association between corticosteroids and intestinal microflora has not been reported, our present results suggest that patients who receive immunosuppressant therapy such as corticosteroids have a potentially high risk for disease exacerbation by H. pylori eradication. Additional study is needed to clarify whether corticosteroids have a unique role in exacerbating IBD at eradication therapy. Emergent H. pylori eradication therapy may be unnecessary in clinical practice, and physicians can therefore avoid H. pylori eradication therapy in IBD patients who receive immunosuppressant drugs. Actually, among patients in the eradication group from whom clinical activity indices were obtained, no severe active patients were included with maximum CDAI and CAI of 176 and 4, respectively. If eradication is necessary for patients with active disease, even though it is mild, careful observation after eradication is advised.
The H. pylori eradication rates in IBD patients in the present study were comparable to previously reported rates for non-IBD patients [23,31,32]. Different acid-suppressive drugs and non-penicillin antibiotics also did not affect the eradication rate, and primary and secondary eradication rates were comparable to previously reported rates for non-IBD patients. These data strengthen our findings that IBD does not affect H. pylori eradication, and provide important information to help physicians select an H. pylori eradication regimen. Moreover, a previous report showed that IBD-related upper gastric lesions, such as focally enhanced gastritis, were not associated with H. pylori infection [33]. Although detailed upper endoscopic findings were not analyzed in the present study, our data strongly indicate that H. pylori infection independently affects upper gastrointestinal lesions associated with IBD.
This study has some limitations. First, as this was a retrospective study, we did not adopt validated disease activity indices for investigating disease exacerbation as the primary endpoint. Second, the analyses for eradicated patients were underpowered due to the limited population under stringent criteria. We then established rigorous inclusion criteria to select patients comprising the non-eradication group, however, a selection bias based on the retrospective study design could not be completely eliminated. And the number of CD patients was considerably smaller than that of UC, which might influence some results. Third, we selected patients in the non-eradication group regardless of H. pylori infection. In the present study we focused on the short-term influences on H. pylori eradication therapy, but not on the long-term effect of IBD patients who succeeded in eradication. To elucidate the long-term influences of H. pylori eradication, another study should be needed to compare more than 1 year clinical courses of H. pylori-infected IBD patients who succeeded in eradication therapy with those who failed in eradication. Finally, in the present study we did not analyze the extent of gastric mucosal atrophy, the H. pylori strain and fecal microbiota. H. pylori strain is broadly divided into Western and East-Asian types based on differences in the cytotoxin associated gene A protein Glu-Pro-Ile-Tyr-Ala motif, which is strongly associated with gastric inflammation and carcinogenesis [34]. A well-designed study in a Western cohort is needed to confirm our results.
In conclusion, we demonstrated that H. pylori eradication therapy does not exacerbate IBD, and does not improve disease activity. Careful observation after eradication therapy is necessary, especially for IBD patients with active disease that undergo eradication therapy.