INTRODUCTION
Ulcerative colitis (UC) is a lifelong immune-mediated inflammatory condition of the colonic mucosa that is characterized by a relapsing and remitting course.1,2 Sustained inflammation in patients with UC results in a progressive worsening of their quality of life.3 Most UC patients are successfully managed with mesalamine formulations, but in approximately 25% of UC patients, mesalamine treatment or other therapies fail, thus requiring intensified treatment or colectomy.4 Corticosteroids remain a mainstay for inducing remission in patients with moderate to severe UC, but their long-term use is not recommended because of adverse side effects.5,6,7 The investigators of one European cohort study that included a large number of UC patients reported that at 1 year after withdrawal of corticosteroid treatment, fewer than half of the patients had a sustained response, one-third required colectomy, and approximately one-fourth required reinduction of corticosteroid treatment due to a UC relapse.8 Thus, the maintenance of steroid-free remission in UC patients is a clinically important issue.
Thiopurines, azathioprine (AZA) and its metabolite 6-mercaptopurine (6-MP) are purine analogs that effectively induce and maintain remission in patients with IBD, particularly in steroid-refractory or steroid-dependent disease.9,10 Although the effects of thiopurine on refractory IBD are apparent in clinical practice, only a few prospective studies and one meta-analysis have been reported.10,11,12 Moreover, little is known about the long-term clinical outcome of UC patients who initially responded to thiopurine treatment.
The efficacy of biologics such as infliximab and adalimumab for induction of remission and maintenance in UC patients has been reported.13,14,15,16 Clinical trials, case series, and a meta-analysis have demonstrated the benefits of these biologic therapies for UC patients.13,14,15,16,17,18,19 The costliness of the long-term use of biologics, however, is problematic.20 In addition, observational data suggest that patients taking biologics are at increased risk of opportunistic infection.21 Therefore, the usefulness of thiopurine for maintaining remission in UC patients must be reconsidered. The aim of this study was to assess the long-term efficacy and safety of maintenance treatment with thiopurine in Japanese patients with UC.
METHODS
1. Study Design
This was a single-center retrospective cohort study. All patients with UC at Kyoto University Hospital who were treated with a thiopurine and 5-aminosalicylate (5-ASA) formulation as maintenance treatment after induction treatments such as 5-ASA, corticosteroids, granulocyte-monocyte adsorption apheresis (GMAA), and calcineurin inhibitors between December 1998 and August 2013 were enrolled in the study. All of the subjects provided informed consent. The study protocol conformed to the Declaration of Helsinki and was approved by the Institutional Review Board at Kyoto University Hospital.
2. Definition of UC
The diagnosis of UC was confirmed by reviewing endoscopic and pathological reports. Disease activity was evaluated based on a modified Truelove and Witts Severity Index (MTWSI) score (Supplemental Table 1).22,23,24 Clinical remission was defined as an MTWSI score lower than 4. UC relapse was defined as an MTWSI score increase of at least 3 points from baseline leading to treatment modification. UC flare-up was defined as an increase in MTWSI score of at least 3 points from the baseline and leading to treatment modification.24 Refractory UC was defined as (1) steroid refractory, or the lack of a clinical response to a systemic daily dose of 30 mg or more of prednisolone over at least 2 weeks; and (2) steroid dependency, or failing to taper the prednisolone dose to less than 10 mg/day within 12 weeks or relapse within 12 weeks after prednisolone discontinuation. Mucosal healing was defined as endoscopic findings with a Mayo score of 0 or 1.13 The time to colonoscopy was different for each patient because this study was retrospective.
To assess mucosal healing, follow-up colonoscopy was routinely performed after clinical remission in UC patients whose corticosteroid dose were completely tapered off.
AZA and 6-MP were administered as thiopurines. We generally administered AZA, and we used 6-MP in patients intolerant to AZA. The thiopurine dose was optimized to achieve a white blood cell count between 3,000 and 5,000/µL or a 6-thioguanine nucleotide concentration between 235 and 450 pmol/8×108 erythrocytes. For UC patients enrolled in this study, induction treatments included 5-ASA, corticosteroids, GMAA, and calcineurin inhibitors such as tacrolimus and cyclosporine. The tacrolimus dose was adjusted to produce consistent trough levels of 10 to 15 ng/mL, and the dose of cyclosporine was adjusted to produce consistent trough levels of 150 to 250 ng/mL.
3. Assessment
The primary endpoint of this study was the remission-maintenance rate with thiopurine and 5-ASA in the UC patients. Secondary endpoints were the predictive factors, namely flare-up, mucosal healing rate, and colectomy-free survival in UC patients treated with thiopurine and 5-ASA.
4. Statistical Analysis
Normally distributed continuous variables were analyzed by using Student's t-test, and nonparametric data were analyzed with Wilcoxon's rank sum test. Categorical variables were analyzed by using Pearson's chi-square test or Fisher's exact test if any cell number was less than 5. A P<0.05 was considered as statistically significant. Cumulative colectomy-free and remission-maintenance rates were assessed by using the Kaplan-Meier method, and groups were compared by using the log-rank test stratified by study. Predictive factors were analyzed with multivariate statistics by using Cox regression. All analyses were performed by using the Statview software (SAS Institute, Cary, NC, USA).
RESULTS
1. Patient Characteristics
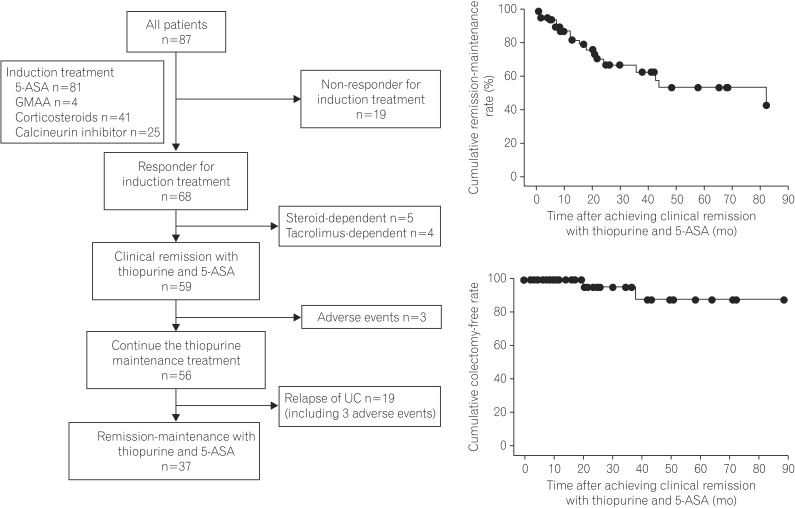
Of the 87 UC patients who received various induction therapies, including 5-ASA, GMAA, corticosteroids, or calcineurin inhibitors, 68 (78.2%) achieved a clinical response with induction treatment and thiopurine. Of the 68 patients, 59 (67.8%) maintained clinical remission with thiopurine and 5-ASA after tapering the dose in the induction treatment (Fig. 1A). Of these 59 patients, 3 (5.1%) discontinued thiopurine treatment because of adverse events, and the remaining 56 patients (94.9%) were evaluated in the present study.
The characteristics of the 56 patients who were undergoing maintenance therapy with thiopurine and 5-ASA are shown in Table 1. Of the 56 patients, 38 (67.9%) were men and 18 (32.2%) were women, with a median age of 31.5 years (range, 13-83 years). The median disease duration from diagnosis of UC to initiation of thiopurine treatment was 33.5 months (range, 1-292 months). Three of the 56 patients (5.4%) had proctitis, 16 (28.6%) had left-sided colitis, and the remaining 37 (66.0%) had extensive colitis. Of the 56 patients, 39 (69.6%) had refractory UC (steroid dependent in 30 patients [76.9%] and steroid refractory in 9 patients [23.1%]). The median MTWSI score at the initiation of the thiopurine treatment was 5.0 points (range, 0-13 points). The median Mayo endoscopic score at the time of thiopurine initiation was 2.0 points (range, 1-3 points). In 52 (94.5%) of the 56 patients, 5-ASA was used for induction treatment. GMAA was used in 4 (7.1%), corticosteroids in 26 (46.4%), and a calcineurin inhibitor (tacrolimus/cyclosporine) in 14 (25.0%).
2. Clinical Remission Maintenance in UC Patients Who Were Receiving Thiopurine and 5-ASA as Maintenance Treatment
Of the 56 patients, 47 (83.9%) were treated with AZA and 9 (16.1%) were treated with 6-MP. The median dose of thiopurine during the maintenance treatment was 50 mg (range, 10-135 mg), although 4 patients (7.1%) received concomitant allopurinol to increase the 6-thioguanine nucleotide concentration. 6-Thioguanine nucleotide concentration was evaluated in 37 (66.1%) of the 56 patients, and the median 6-thioguanine nucleotide concentration was 358.8 pmol/8×108 erythrocytes (range, 50-1,670 pmol/8×108 erythrocytes). In addition, 52 (94.5%) of the 56 patients received concomitant 5-ASA, and the median 5-ASA dose was 3,000 mg (range, 250-4,000 mg) during thiopurine maintenance treatment.
Of the 56 patients, 37 (66.1%) were maintained in clinical remission with thiopurine and 5-ASA (remission group), while 19 (33.9%) had a UC relapse during the study period (relapse group). Six UC patients discontinued thiopurine due to adverse events. However, 3 of them experienced a UC relapse at the onset of adverse events and were included in the relapse group (Fig. 1A). The median follow-up duration after initiating thiopurine in the 56 patients who achieved clinical remission was 33.0 months (range, 4-143 months). Based on the Kaplan-Meier analysis, the cumulative remission-maintenance rates in the 56 patients treated with thiopurine and 5-ASA after the dose in the induction treatment was tapered were estimated to be 43.9% at 84 months, 94.3% at 6 months, 84.6% at 12 months, 69.0% at 24 months, 54.9% at 48 months, 54.9% at 72 months, and 43.9% at 84 months, respectively (Fig. 1B).
3. Predictive Factors of Maintaining Remission With Thiopurine
To evaluate the predictive factors of maintaining remission with thiopurine, we evaluated the differences in the patient characteristics between the remission and relapse groups. The number of UC patients with a history of corticosteroid use (≥40 mg/day) differed significantly between the remission and relapse groups (Table 1). According to the Kaplan-Meier analysis, the cumulative remission-maintenance rate was significantly lower in the UC patients with than in those without a history of treatment with a corticosteroid dosage ≥40 mg/day (12.1% at 83 months vs. 51.5% at 84 months, P=0.032). Moreover, the multivariate analysis using Cox regression suggested that history of treatment with a corticosteroid dosage ≥40 mg/day was indicated as a negative predictive factor of clinical remission maintenance in UC patients (hazard ratio, 3.76; P=0.01) (Table 2).
4. Mucosal Healing for UC Patients Receiving Maintenance Treatment With Thiopurine and 5-ASA
Of the 56 UC patients, 38 (67.9%) underwent colonoscopy to evaluate mucosal healing, and the median time to assessing mucosal healing after initiating thiopurine agents was 26.8 months (range, 1-84 months). Among the 38 patients, 23 (60.5%) achieved mucosal healing (mucosal healing group) and 15 (39.5%) did not achieve mucosal healing (non-mucosal healing group). To evaluate the predictive factors of mucosal healing in the UC patients who maintained clinical remission with thiopurine, we analyzed the differences in patient characteristics between the mucosal and non-mucosal healing groups. The serum CRP concentration and number of UC patients with a history of corticosteroid treatment ≥40 mg/day tended to be greater in the non-mucosal healing group than in the mucosal healing group, although no significant differences in patient characteristics were observed between the mucosal and non-mucosal healing groups (Table 3). Based on the multivariate analysis (Table 4), CRP elevation was a negative factor of mucosal healing (hazard ratio, 1.46; P=0.03).
5. Colectomy-Free Rate Among UC Patients Who Achieved Steroid-Free Remission With Thiopurine and 5-ASA
Of the 56 patients, 2 (3.6%) underwent colectomy due to a UC relapse under steroid-free remission. Based on the Kaplan-Meier analysis, the estimated cumulative colectomy-free rate of the UC patients whose remission was maintained with thiopurine was 88.0% at 84 months (Fig. 1C).
6. Adverse Events
Adverse events occurred in 17 (28.8%) of the 59 patients who achieved clinical remission with thiopurine and 5-ASA (Table 5). Moreover, 6 (10.2%) of the 59 patients discontinued thiopurine treatment because of adverse events. Adverse events requiring withdrawal of thiopurine treatment included infectious mononucleosis (1 patient, 1.7%), nausea (1 patients, 1.7%), liver dysfunction (2 patients, 3.4%), pancreatitis (1 patient, 1.7%), and leukopenia (1 patients, 1.7%). All of the patients recovered from adverse events upon discontinuation of thiopurine, and no mortality due to adverse events occurred during the follow-up.
DISCUSSION
The findings of the present study demonstrate the long-term efficacy and safety of thiopurine for maintaining remission in bio-naive UC patients. A history of treatment with high-dose corticosteroids affects both the maintenance of remission and mucosal healing in bio-naive UC patients treated with thiopurine.
Recently, many papers reported the efficacy of biologics for the induction and maintenance of remission in refractory UC patients.13,14,15,16,17,18,19 Induction and maintenance of long-term remission in patients with mild to moderate bio-naive UC, however, should also be considered. Controlled studies have demonstrated that thiopurines are effective for steroid tapering and maintenance of remission in UC patients.11 Several meta-analyses also demonstrated the efficacy of thiopurine for the induction and maintenance of remission in UC.9,10,11,12,25,26 In the present study, clinical remission was maintained with thiopurine in 66.1% of the bio-naive UC patients, suggesting the high efficacy of thiopurine for maintenance of remission in UC patients.
The identification of UC patients in whom clinical remission can be maintained with thiopurine is highly important for long-term treatment of UC. Nquyen et al. reported that factors such as age, sex, patient adherence, duration of treatment with thiopurine, erythrocyte count, and erythrocyte sedimentation rate could not predict the efficacy of thiopurine.27 Interestingly, our data revealed that corticosteroid treatment, particularly in those with a history of high-dose corticosteroid use, might be a negative predictive factor of maintaining remission with thiopurine in UC patients. Thus, high-dose corticosteroids should be avoided for successful management of UC patients.
The aims of UC treatment should include the promotion of mucosal healing and the induction and maintenance of clinical remission, because several reports indicate that mucosal healing reduces the rate of hospitalization and colectomy, improving patient quality of life.13,28,29 Data regarding the usefulness of thiopurine for achieving and maintaining mucosal healing in UC patients, however, are limited. In a cohort study with a small number of UC patients reported by Lopez et al., 60% of UC patients who maintained remission with thiopurine also achieved and maintained mucosal healing.28 Endoscopic activity might be predictive of flare-up in UC patients, even if clinical remission is maintained. The present study revealed that the mucosal healing rate in UC patients who maintained remission with thiopurine treatment (60.5%) was similar to that in the study of Lopez et al.28 and suggests that a high CRP concentration is a negative predictor of mucosal healing. Previous studies demonstrated the positive correlation between CRP level and the drgree of mucosal inflammation evaluated by using endoscopy, especially in severe UC.30,31,32 High doses and long-term use of corticosteroids could affect epithelial regeneration by inhibiting nuclear factor kappa B activation in epithelial cells,33 even if thiopurines are selected for maintenance treatment. In this regard, the use of high-dose corticosteroids for the treatment of UC should be avoided as much as possible.
Previous reports indicated that treatment with thiopurine may increase the risk of life-threatening adverse events, particularly malignancies.34,35,36,37 The guidelines of the European Crohn's and Colitis Organization, however, recommend thiopurine as a first-line treatment for refractory UC patients who experience a UC flare-up during corticosteroid withdrawal.38 In the present study, adverse events occurred in 27.1% of the UC patients treated with thiopurine. The frequency of adverse events in our study was similar to that in previous reports26,34,35 Moreover, no life-threatening infections or malignancies occurred in the observational period (7 years). Roblin et al.39 reported that an optimal dose of thiopurine might help to prevent severe adverse events. Therefore, monitoring 6-thioguanine nucleotide levels is required for maintenance of long-term remission and the prevention of adverse events in UC patients treated with thiopurine.
The present study has several limitations, including the small number of patients and the single-center, retrospective design. In addition, the time to assess endoscopic activity after achieving clinical remission varied. Therefore, our data should be interpreted with caution, and further studies with a larger number of enrolled patients are required.
In conclusion, our long-term observational data indicate that thiopurine is useful for maintaining remission and promoting mucosal healing in bio-naive UC patients. Optimal use of thiopurine will contribute to long-term remission in bio-naive UC patients.