INTRODUCTION
The prognosis of patients with gastric cancer has improved with detection at early stages and advances in treatment modalities [1,2]. Therefore, detection of secondary cancer is as important as surveillance of gastric cancer recurrence. Colorectal cancer (CRC) has been recognized as the most common synchronous malignancy in patients with gastric cancer [3-5]. The prevalence of concomitant CRC at the time of surgical or endoscopic treatment in gastric cancer patients was reported as 1%-4% [3-6]. Although the prevalence of colorectal neoplasms (CRN) including CRC was higher in patients with gastric cancer than in healthy individuals, most studies have investigated the prevalence of concomitant CRN at the time of surgical resection or endoscopic resection of gastric cancer. CRC develops from benign CRN through the adenoma-carcinoma sequence [7]. Regular surveillance colonoscopy based on the number and histology of resected CRN is recommended after resection of CRN [8,9]. No previous study has investigated the prevalence of CRN after surgical treatment of gastric cancer. In this study, we aimed to investigate whether CRN was more prevalent in gastric cancer patients after surgical treatment than in healthy individuals.
METHODS
Among a cohort of gastric adenocarcinoma patients who underwent gastrectomy at Incheon St. Mary’s Hospital (Incheon, Republic of Korea), we reviewed the medical records of consecutive subjects who underwent colonoscopy between January 2016 and December 2017 [10]. We excluded patients with cecal intubation failure; or inadequate bowel preparation. Colonoscopy was performed at least 1 year after gastrectomy. In our center, colonoscopy for gastric cancer patients is included in the routine staging work-up before surgery [11]. Therefore, most gastric cancer patients undergo colonoscopy before surgery. The control group comprised healthy subjects who underwent colonoscopy at the health-care center of our institution during the study period and were matched with gastric cancer patients by age and sex in a 2:1 ratio. Demographic characteristics, bowel preparation quality, and results of colonoscopy were investigated. Cancer staging and type of surgery were investigated in the gastric cancer group. Cancer staging was performed at the time of gastrectomy using the 7th edition of the American Joint Committee on Cancer Staging Manual [12].
1. Colonoscopic Examinations
Colonoscopy was performed by 3 attending physicians with more than 4 years of experience using an Olympus (Olympus, Seoul, Korea) series Q260 or Q290 colonoscope [13,14]. Bowel preparation was done with 4 L of polyethylene glycol. To obtain optimal bowel cleansing, patients were instructed to ingest additional liquid until no solid particles were observed in the bowel effluent [15]. Bowel cleansing quality was assessed using the Aronchick scale [16,17]. Polyp resection was performed during withdrawal of the colonoscope. The colonoscopists were encouraged to observe the colonic mucosa for at least 6 minutes [18]. Polyp resection was performed by cold snare polypectomy or conventional endoscopic mucosal resection at the physician’s discretion. Histologic assessment of resected polyps was performed by specialist gastrointestinal pathologists. Cecal intubation time, colonoscope withdrawal time, and total colonoscopy time were analyzed. Colonoscope withdrawal time was determined as the time difference between photographic documentation of the cecum and anus in patients who did not undergo any procedures such as a biopsy or polypectomy [19].
2. Definition
CRN included adenomas or cancers but excluded nonneoplastic lesions (hyperplastic, lymphoid, inflammatory). Advanced CRN (ACRN) was defined when one of the following criteria was met: (1) adenocarcinoma; (2) adenoma sized at least 1 cm; (3) the presence of at least 3 adenomas; and (4) the presence of villous adenoma or high-grade dysplasia [8,20]. The rate of CRN, ACRN, and CRC and the number of adenomas per patient were analyzed. The protocol of this study was approved by the Institutional Review Board of Incheon St. Mary’s Hospital (IRB No. OC17MES0031). Written informed consent was obtained from all patients.
3. Statistical Analysis
All statistical analyses were performed using IBM SPSS version 20 (IBM Corp., Armonk, NY, USA). Continuous variables were compared using Student t-test or the Mann-Whitney test when appropriate. Categorical variables are presented as number (percent) and compared using the chi-square or Fisher exact tests. We compared the clinical data and prevalence of (A)CRN and CRC between the gastric cancer and the control group. To investigate the factors contributing to having (A) CRN or CRC, we compared the clinical data of all the patients with and without (A)CRN or CRC. Logistic regression modeling was used to perform multivariate analysis of risk factors for (A)CRN or CRC that were found to be significant in the univariate analysis. Odds ratio (OR) and 95% confidence interval (CI) were calculated for the prevalence of (A)CRN and CRC. A P-value < 0.05 was considered significant.
RESULTS
Two hundred and sixty-six patients with gastric cancer underwent colonoscopy during the study period. Of these patients, 18 were excluded because of cecal intubation failure (n = 5) or inadequate bowel preparation (n = 13). After matching of healthy subjects, a total of 744 patients were finally included in this study: gastric cancer (n = 248) and healthy control (n = 496). The demographic and clinical data of the 2 groups are shown in Table 1. Age, sex, comorbidities, family history of CRC, and factors related to previous colonoscopy were similar between the 2 groups. Body mass index was lower in the patients with gastrectomy (gastric cancer group 21.3 kg/m2 vs. control group 24.4 kg/m2, P<0.001). Indications for colonoscopy differed between the 2 groups (P<0.001). The median interval between surgery and colonoscopy in the gastric cancer group was 51 months.
1. Prevalence of CRN
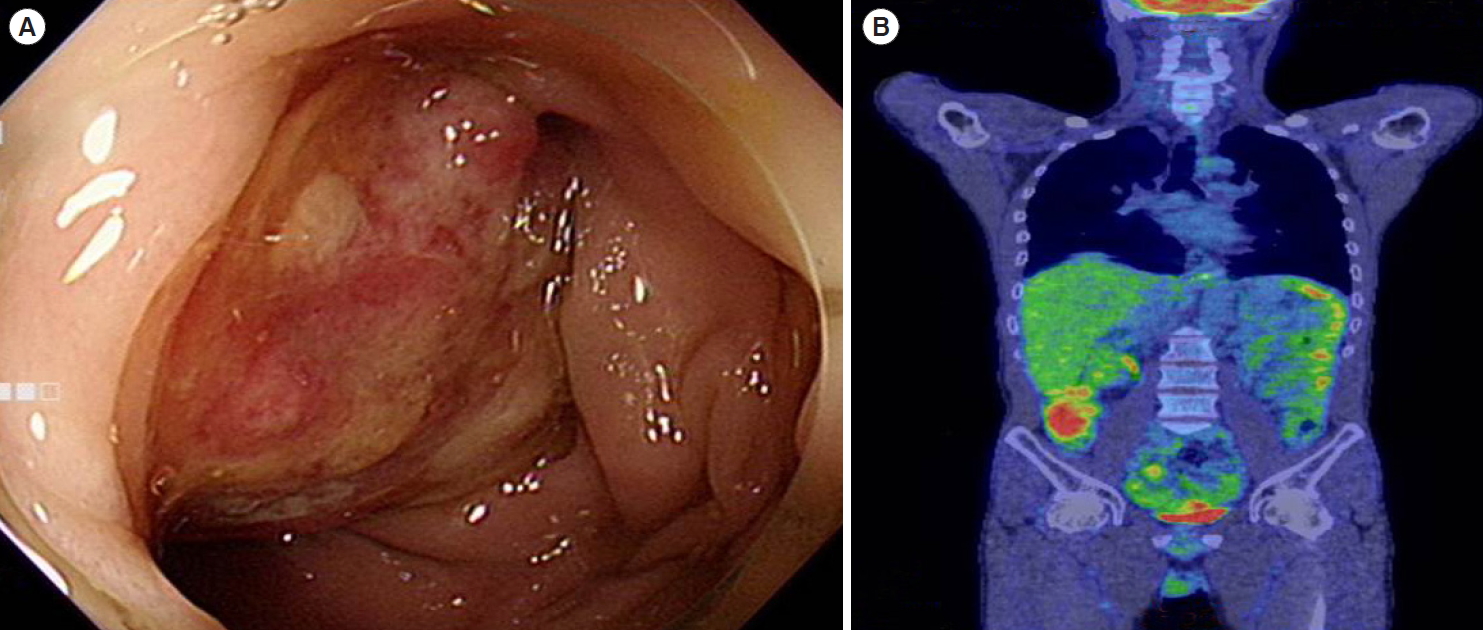
The rate of polyp detection in the gastric cancer group was 55.6%, which was higher than that in the control group (46.4%, P=0.017). The prevalence of CRN and ACRN in the gastric cancer group was higher than that in the control group (CRN: 47.6% vs. 34.7%, OR, 1.710; 95% CI, 1.254-2.332; P<0.001 and ACRN: 16.9% vs. 10.9%, OR, 1.669; 95% CI, 1.079-2.580; P=0.020) (Table 2, Fig. 1). However, the rate of CRC was comparable between the 2 groups (gastric cancer 2% vs. control 0.6%, P=0.125). The rate of sessile serrated adenoma/polyp was comparable between the 2 groups (2.4% vs. 2.0%, P=0.721). The mean number of adenomas per patient was comparable between the 2 groups (gastric cancer 0.9 vs. control 0.7, P=0.833). Metastatic cancer was found in 3 gastric cancer patients (Fig. 2). In the gastric cancer group, the rate of CRN (stage I 48.8% vs. stage II+III 45.2%, P=0.597), ACRN (stage I 15.2% vs. stage II+III 20.2%, P=0.321) and CRC (stage I 1.2% vs. stage II+III 3.6%, P=0.340) was not higher in the advanced cancer stage. However, all metastatic cancer was found in gastric cancer with stage III.
2. Results of Colonoscopy
The details of colonoscopy are shown in Table 2. The time needed for colonoscope insertion was longer in the gastric cancer group than in the control group (gastric cancer 5.0 minutes vs. control 3.9 minutes, P<0.001). Withdrawal time was comparable for both groups (gastric cancer 6.8 minutes vs. control 6.7 minutes, P=0.386). Total colonoscopy time was longer in the gastric cancer patients (gastric cancer 16.8 minutes vs. control 14.1 minutes, P<0.001). Overall bowel cleansing efficacy in the control group was superior to that in the patients with gastrectomy (P<0.001). Perforation or postpolypectomy bleeding did not occur in either group.
3. Risk Factors for CRN
Male sex and a history of gastrectomy were significant risk factors for CRN in univariate analysis (Table 3). The patients with CRN were older than those without CRN (CRN 63.2 years vs. without CRN 61.9 years, P=0.042). Multivariate analysis revealed that male sex (OR, 2.183; 95% CI, 1.590-2.996) and a history of surgery for gastric cancer (OR, 1.748; 95% CI, 1.274-2.400) were significant risk factors for CRN. A comparison of individuals with and without ACRN is shown in Table 4. Univariate analysis revealed that male sex and a history of gastric cancer were significant risk factors for ACRN. After multivariate analysis, male sex (OR, 3.620; 95% CI, 2.092-6.265) and a history of surgery for gastric cancer (OR, 1.705; 95% CI, 1.094-2.659) were identified as significant risk factors. There was no significant difference between patients with and without CRC.
DISCUSSION
To our knowledge, this study is the first to investigate the usefulness of colonoscopy in gastric cancer patients after gastrectomy. This study confirmed that CRN and ACRN were more prevalent in patients with gastric cancer after gastrectomy than in healthy individuals.
Known risk factors for CRC are diabetes, hyperlipidemia, alcohol use, and a diet rich in animal fat [21,22]. The incidence of CRC has been reported to be inversely proportional to the consumption of nonsteroidal anti-inflammatory drugs (NSAIDs) and aspirin [22]. Our group previously investigated the usefulness of screening colonoscopy in gastric cancer patients before surgery [11], and showed that CRN, ACRN, and CRC were more prevalent in the gastric cancer group than in healthy controls. Although CRC is the most common synchronous cancer with gastric cancer, the relationship between these 2 cancers has not been determined. Several studies have suggested that Helicobacter pylori, a causative organism of gastric cancer, is also a risk factor for CRC [23,24]. In the current study, we compared the prevalence of CRN, ACRN, and CRC between postgastrectomy gastric cancer patients and healthy individuals. The prevalence of CRC was numerically higher in the gastric cancer patients than in the control group, but this difference was not significant. The prevalence of CRN and ACRN was significantly higher in the gastric cancer group than in the healthy controls. In the multivariate analysis, gastric cancer was an independent risk factor for CRN and ACRN. This indicates that regular scheduled colonoscopy should be performed after gastrectomy.
In the current study we excluded patients who underwent endoscopic resection. In a previous study, the prevalence of CRN at the time of resection did not differ between the patients who underwent surgical resection and endoscopic resection [11]. Colonoscopy in patients who underwent gastrectomy is technically demanding because of bowel adhesion. In our center, colonoscopy before gastrectomy and follow up colonoscopy after surgery was usually performed by fellows (gastroenterologist and surgeon). However, in the current study, the colonoscopy in both groups was performed by same experience colonoscopists (professor of gastroenterology) who are low risk for missing adenoma or having chance of interval cancer.
Guidelines recommend an initial screening test for CRC in the general population, starting at age 50, using a stool-based test or endoscopy including colonoscopy and sigmoidoscopy [18]. Colonoscopy is recognized as the best diagnostic method for detecting CRC and has several benefits. First, as well as detecting CRC, colonoscopy can simultaneously treat a precancerous CRN at the time of diagnosis and hence can prevent CRC [25]. Most CRNs found at colonoscopy are less than 1 cm in diameter, and are suitable for conventional methods of polypectomy including hot or cold snare polypectomy [26,27]. Second, colonoscopy can detect metastatic cancer after gastrectomy. We identified metastatic cancer in 3 patients in the gastric cancer group.
We also compared colonoscopy quality measures between the 2 groups. The colonoscope insertion time was longer in the patients who underwent gastrectomy. Colonoscope insertion time is an important technical measure of colonoscopy [28]. Although the technical difficulty of colonoscope insertion was not recorded by the colonoscopists, the longer insertion time in the gastric cancer group indirectly suggests that colonoscope insertion was more technically demanding in postgastrectomy patients than in the healthy population. We investigated colonoscope withdrawal time only in patients who did not undergo any additional procedures such as a biopsy or polypectomy. Colonoscope withdrawal time is usually defined as the mucosal inspection time excluding time for fluid suction or additional procedures. Thus, it was challenging to analyze colonoscope withdrawal time accurately in patients who underwent polypectomy or a biopsy. In previous studies, the mean inspection time for upper endoscopy or colonoscopy was defined as the amount of time that did not result in any positive finding that required additional procedures [19,29]. In the current study, colonoscope withdrawal time was comparable between the 2 groups. The rate of adenoma detection has been reported to be influenced by withdrawal time, which is an important indicator of adequate colonoscopy [27].
We acknowledge several limitations of the current study. First, because of its retrospective design, several patients had missing data. Colonoscope withdrawal time was measured in only 50% of the patients. However, colonoscopy for both groups was performed by the same colonoscopists and withdrawal time was similar for both groups. The use of medications such as aspirin or NSAIDs, which are known to have a protective effect against CRC development, was not analyzed. Second, the control subjects were matched from those who underwent colonoscopy at a health-promotion center, who were relatively healthy and had a strong interest in health screening. Indications for colonoscopy and bowel cleansing quality differed between the 2 groups. A previous history of abdominal surgery is a risk factor for suboptimal bowel cleansing [30]. However, we excluded patients with inadequate bowel cleansing and therefore believe that these parameters did not affect the main outcome of our study. Third, this study was not designed to investigate the rate of CRN in the gastric cancer group and the control group.
Despite the limitations described above, our study has several strengths. First, using a well-preserved cohort of surgical data, we included consecutive gastric cancer patients who underwent colonoscopic examination during the study period. Second, colonoscopic examination was performed by experienced endoscopists and quality measures for colonoscopy were met. The rate of adenoma detection was more than 25% and colonoscope withdrawal time was longer than 6 minutes for both groups.
In conclusion, our study demonstrated that CRN and ACRN were more prevalent in postgastrectomy gastric cancer patients than in healthy individuals. A history of surgery for gastric cancer was an independent risk factor for CRN and ACRN. The results of the current study address the importance of regular surveillance colonoscopy after gastrectomy at appropriate intervals. Future clinical trials are needed to validate the results of this study.