Magnetic resonance enterography predicts the prognosis of Crohn's disease
Article information
Abstract
Background/Aims
Magnetic resonance enterography (MRE) has emerged as an important tool in the diagnosis and follow-up of Crohn's disease (CD). The aim of this study was to evaluate whether MRE findings could predict the prognosis of CD.
Methods
In this retrospective study, a total of 173 patients with clinical remission of CD (n=61) or active CD (n=112) were identified. The outcomes of clinical relapse, admission, surgery, and need for other medications according to the MRE findings were evaluated.
Results
The presence of active inflammation on MRE was observed in 93 (83%) patients with clinically active CD and in 44 (72.1%) patients with clinical remission of CD, without a statistically significant difference (P=0.091). In multivariate analysis, active inflammation on MRE increased the risk for clinical relapse (hazard ratio [HR], 6.985; 95% confidence interval [CI], 1.024–47.649) in patients with clinical remission of CD. In patients with clinically active CD, active inflammation on MRE increased the risk for CD-related hospitalization (HR, 2.970; 95% CI, 1.006–8.772).
Conclusions
The presence of active inflammation on MRE was significantly associated with poor prognosis both in patients with clinical remission of CD and in those with active CD.
INTRODUCTION
Crohn's disease (CD) is a chronic transmural IBD that can occur throughout the gastrointestinal tract. It is characterized by repeated episodes of exacerbation and regression. Approximately 70% of patients with CD have small-bowel involvement, and 30% of them have disease limited to the small bowel.1 Mucosal healing has become the treatment target in the management of CD.2 However, it is difficult to recognize mucosal lesions in patients with small-bowel lesions using conventional endoscopic methods. The CDAI is widely used in assessing disease activity; however, clinical symptoms scored by CDAI are not reliable measures of mucosal inflammation.3 Computerized tomography enterography (CTE) imaging is useful for assessing disease activity in CD but exposes patients to a large dose of radiation during each evaluation, therefore preventing repeated examinations.4
In recent years, magnetic resonance enterography (MRE) has emerged as an important tool in the diagnosis and follow-up of CD.5 MRE can provide information on the deep small intestine and extraluminal manifestations of CD.6 MRE is preferred because it does not expose patients to ionizing radiation, has a high tissue contrast, and uses safe gadolinium-based contrast media.7 A correlation between MRE imaging and the disease activity of CD has been established.8 In a meta-analysis study, the sensitivity and specificity of MRI for the detection of CD were found to be 93.0% and 92.8%, respectively.9 In other study, MRE detected ulcerative lesions in the small intestine with 82.4% sensitivity and 87.6% specificity.10 In another study assessing ileocolonic CD, MRE imaging was superior to CTE in detecting intestinal strictures and ileal wall enhancement.11
In a recent study, Deepak et al.12 revealed that radiological response detected with CTE or MRE was associated with a reduction in the long-term risk of hospitalization, surgery, or corticosteroid use among patients with small-bowel CD. However, few studies have evaluated the prognosis of patients with CD in terms of the first MRE findings both at the time of clinical remission and during the clinically active state. Therefore, the purpose of our study was to evaluate the usefulness of MRE imaging in assessing the prognosis of CD. We hypothesized that active inflammatory findings on MRE would be associated with poor prognosis such as relapse, admission, surgery, need for corticosteroids, need for adding other medications, or need for increasing the dose of current medications even in patients with clinical remission of CD.
METHODS
1. Patients
In this retrospective study, we reviewed the medical records of patients with CD who underwent MRE imaging at Severance Hospital, Yonsei University College of Medicine, Seoul, Korea, between December 2012 and March 2016. The purposes of MRE imaging evaluation were divided into 2 categories: evaluation of current CD activity at the time of clinical remission and that during the clinically active state. MRE was performed in order to follow-up after the treatment. The indications for MRE were when the symptoms persisted despite treatment, complications were suspected, inflammatory markers were elevated even with clinical remission, and determination of the appropriateness of current treatment. The CDAI according to the criteria of Best et al.13 was used to assess the disease activity of patients with CD. A CDAI score <150 was considered to indicate clinical remission. Clinical relapse was defined as the occurrence or worsening of symptoms, accompanied by an increase in the CDAI score to >150.14
Descriptions of patient age at CD diagnosis, disease location, and phenotype were based on the Montreal classification.15 Previous surgery was defined as a prior CD-related surgery that includes major surgeries such as ileocecectomy and small-bowel resection. The exclusion criteria were patient age <18 years, inaccurate diagnosis of CD, <3 months of follow-up, and any contraindications to MRE imaging such as the presence of a pacemaker in patients.
Admission was defined as hospitalization for >1 day through the emergency room or outpatient clinic. Surgery was defined as any CD-related surgeries such as small-bowel resection and ileocecectomy. The need for corticosteroids was defined as the addition of any amount of corticosteroids in patients who were not steroid users during the follow-up period after MRE examination. The need for adding other medications or increasing the dose of current medications was defined as the addition of another type of CD medication or increasing the dose of medications used after MRE examination including corticosteroids, respectively. The study was approved by the Institutional Review Board of Severance Hospital (IRB No. 4-2016-0857) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived.
2. MRE Technique
We used very low concentration of barium suspension (easy Mark 0.1; Taejoon Pharmaceutical, Seoul, Korea) for luminal distension of small bowel. Patients were given 1,350 mL of this solution orally 60 minutes before MRI. A 3-T imaging unit (Achieva 3T; Philips, Best, the Netherlands or Discovery 750; GE Healthcare, Milwaukee, WI, USA) was used. Briefly, the following sequences were performed: coronal T2-weighted half-Fourier sequences with and without fat suppression; coronal and axial T2-like steady-state gradient-echo sequences with fat suppression; coronal free breathing diffusion-weighted imaging (with b factors of 0, 500, and 800 s/mm2) and apparent diffusion coefficient mapping; and coronal T1-weighted spoiled gradient-echo sequences with fat suppression, including unenhanced imaging and dynamic phases sequences performed after intravenous administration of gadolinium-based contrast material (Gadovist; Schering, Berlin, Germany) (0.2 mmol/kg at a rate of 2 mL/s) followed by a saline bolus injection and an axial delayed contrast-enhanced T1-weighted spoiled gradient-echo sequence with fat suppression. To avoid bowel peristalsis, 10 mg scopolamine-N-butyl bromide (Buscopan; Boehringer-Ingelheim, Ingelheim, Germany) was administered intravenously, immediately before imaging. An additional same dose of scopolamine was injected immediately before the contrast-enhanced T1-weighted imaging.
3. Image Analysis
The MRE images were reviewed retrospectively by 2 experienced radiologists (J.S.L. and N.S.) who were blinded to the clinical and laboratory findings of the patients. Active inflammation on MRE was defined as the presence of more than one of the following findings: mural thickening >3 mm, mural hyperenhancement, mural edema (increased signal intensity on T2-weighted images), comb sign (sign of engorged vasa recta), penetration (sinus tract, fistula, abscess), or restricted diffusion on diffusion-weighted images.1617181920 Mucosal healing was defined as the absence of any findings of active inflammation.
4. End Points
The end points were the rates of clinical relapse, admission, surgery, need for corticosteroids, need for adding other medications, or need for increasing the dose of current medications according to the purpose of the MRE examination.
5. Statistical Analysis
Statistical analyses were conducted by using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were compared by using the two-sample t-test or the Mann-Whitney U-test. The chi-square test or Fisher exact test was used to analyze categorical data. The cumulative probabilities of clinical relapse, admission, CD-related surgery, need for corticosteroids, need for adding other medications, or need for increasing the dose of current medications were estimated by using the Kaplan-Meier method and the log-rank test. A Cox proportional hazards model was used for assessing the risk of clinical relapse, admission, CD-related surgery, need for corticosteroids, need for adding other medications, or need for increasing the dose of current medications. A P-value of <0.05 was considered statistically significant.
RESULTS
A total of 173 consecutive patients with CD who met the inclusion criteria were included in this study (Fig. 1). The baseline characteristics of the patients on the day of MRE examination are summarized in Table 1. There were 127 male (73.4%) and 46 female (26.6%) patients whose median age at diagnosis was 21 years (interquartile range [IQR], 18–27 years). The median BMI was 20 kg/m2 (IQR, 18–22 kg/m2), and the median duration of disease was 7 years (IQR, 4–11 years).
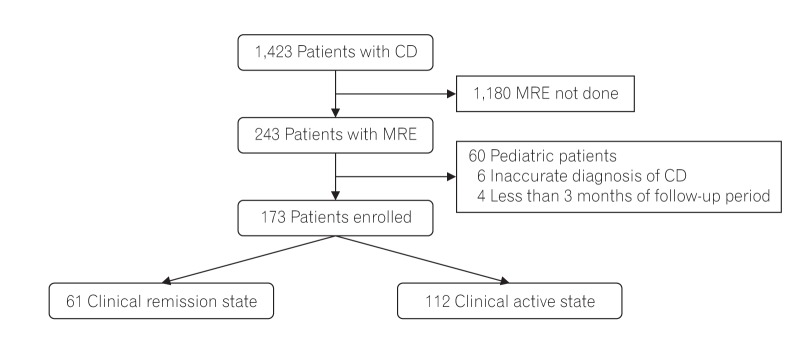
Recruitment algorithm. A total of 243 consecutive patients with magnetic resonance enterography (MRE) were enrolled. After 70 patients were excluded according to our exclusion criteria, a total of 173 patients were selected for statistical analysis.

Baseline Characteristics of Patients with CD on the Day of MRE Examination
The median CDAI on the day of MRE examination was 95 (IQR, 61–122) in patients with clinical remission of CD and 228 (IQR, 187–277) in patients with clinically active CD (P<0.001). The median CRP level and ESR were higher in patients with clinically active CD than in those with clinical remission of CD (P<0.001 and P=0.003, respectively), and the median albumin level was lower in patients with clinically active CD (P<0.001). Almost half of the patients (49.7%) had perianal lesions, and 71 patients (41%) had a previous CD-related surgery. The median follow-up period after MRE was 14.4 months (IQR, 9.9–20.1 months) in patients with clinical remission of CD and 17.7 months (IQR, 12.3–22.9 months) in those with clinically active CD (P<0.001).
The presence of active inflammation on MRE was observed in 93 (83.0%) patients with clinically active CD and in 44 (72.1%) patients with clinically remission of CD, with no statistically significant difference (P=0.091). More than 72% of patients with clinical remission of CD still had active inflammation on MRE examination.
A total of 61 patients were in the clinical remission state, and their baseline characteristics according to the MRE results are detailed in Table 2. Forty-four patients (72.1%) had active inflammation on MRE, and their median CRP was higher than that of patients with no active inflammation on MRE (P=0.003). The median albumin level was significantly lower in the group with active inflammation than in the group without (P=0.008).

Baseline Characteristics of Patients with Clinical Remission of CD: Comparison between Patients with and Those without Active Inflammation
A total of 112 patients were in the clinically active state, and their baseline characteristics are summarized in Table 3. The median CRP level and ESR were higher in the group with active inflammation (P<0.001 and P<0.001, respectively), and the median albumin level was higher in the group without active inflammation (P<0.001).

Baseline Characteristics of Patients with Clinically Active CD: Comparison between Patients with and Those without Active Inflammation
1. Medication Use
The medications used at the time of MRE examination among patients with clinical remission of CD were 5-aminosalicylic acid (5-ASA) in 56 patients (91.8%), azathioprine in 34 patients (55.7%), tumor necrosis factor α (TNF-α) inhibitors in 10 patients (16.4%), corticosteroids in 1 patient (1.6%), methotrexate in 1 patient (1.6%), and none in 1 patient (1.6%). Among 61 patients in the clinical remission state, the need for adding other medications or increasing the dose of current medications was observed in 24 patients (39.3%), and of these, addition of corticosteroids was observed in 5 patients (8.2%).
The medications used at the clinically active state of CD were 5-ASA in 95 patients (84.8%), azathioprine in 64 patients (57.1%), TNF-α inhibitors in 27 patients (24.1%), corticosteroids in 7 patients (6.3%), methotrexate in 2 patients (1.8%), and none in 1 patient (0.9%). Among 112 patients with clinically active CD, the need for adding other medications or increasing the dose of current medications was observed in 77 patients (68.8%), and addition of corticosteroids was observed in 37 patients (33%).
2. Outcomes of Patients with Clinical Remission of CD
In multivariate analysis, active inflammation on MRE increased the risk for relapse (hazard ratio [HR], 6.985; 95% CI, 1.024–47.649), and the risk for the need for adding other medications or increasing the dose of current medications (HR, 6.440; 95% CI, 1.432–28.966) in patients with clinical remission of CD (Table 4). The age at diagnosis of CD and the median albumin level were related to the risk for the need for adding other medications or increasing the dose of current medications. In the Kaplan-Meier analysis with the log-rank test, the presence of active inflammation on MRE imaging was significantly associated with higher cumulative probabilities of relapse (P=0.025), or the need for adding other medications or increasing the dose of current medications (P=0.029), compared with the absence of active inflammation on MRE (Fig. 2).

Univariate and Multivariate HR for Relapse and Need for Adding Other Medications or Increasing the Dose of Current Medications in Patients with Clinical Remission of CD
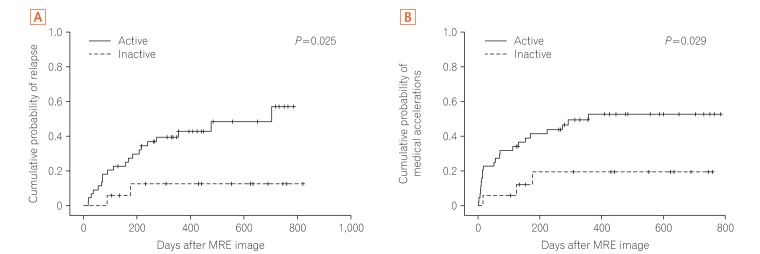
Cumulative probabilities of a change in relapse (A) and the need for adding other medications or increasing the dose of current medications (B) according to magnetic resonance enterography (MRE) findings at the time of clinical remission.
3. Outcomes of Patients with Clinically Active CD
In multivariate analysis, active inflammation on MRE increased the risk for CD-related admission (HR, 2.970; 95% CI, 1.006–8.772) in patients with clinically active CD (Table 5). According to the Montreal classification, patients who were diagnosed as having CD at age between 17 and 40 years (A2) had a lower risk for the need for corticosteroids (HR, 0.413; 95% CI, 0.185–0.923) and for adding other medications or increasing the dose of current medications (HR, 0.373; 95% CI, 0.197–0.707). Stricturing disease (B2) (HR, 2.383; 95% CI, 1.005–5.383) or penetrating disease (B3) (HR, 2.795; 95% CI, 1.207–6.476) increased the risk for admission, compared with nonstricturing or nonpenetrating disease (B1). Penetrating disease (B3) increased the surgical risk (HR, 5.454; 95% CI, 1.094–27.178), and structuring disease (B2) showed a trend toward an increased risk of surgery (P=0.056). The cumulative probability of admission (P=0.009) was higher in patients with active inflammation on MRE imaging than in those without (Fig. 3).

Univariate and Multivariate HR for Admission in Patients with Clinically Active CD
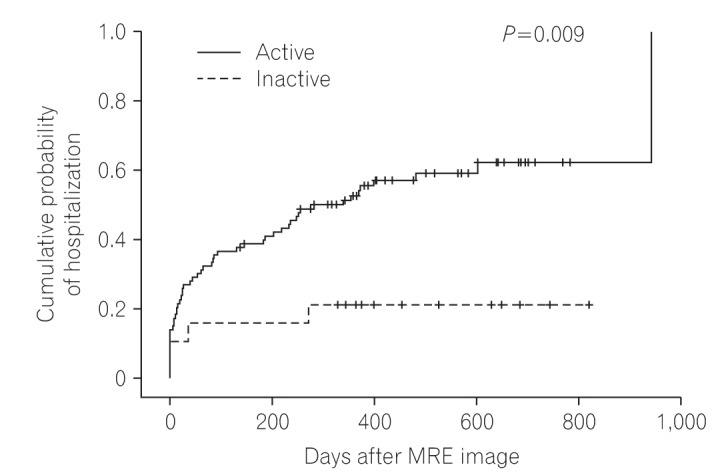
Cumulative probabilities of a change in admission according to the magnetic resonance enterography (MRE) findings during the clinically active state.
DISCUSSION
Regular evaluation of disease activity in patients with CD is important to allow providing adequate medical or surgical therapy, and monitoring drug efficacies.212223 Until recently, the goal of therapy for CD was only to eliminate disease-related symptoms, improve the quality of life of patients, and maintain general wellness by minimizing adverse effects and long-term sequelae.24 In recent studies, the efficacy of CDAI as an indicator of disease severity has been found to be inconclusive.2526 In our study, the CDAI score was not well correlated with the risk for relapse, surgery, or the need for other medications, except for the risk of admission (HR, 1.005; 95% CI, 1.000–1.009) in patients with clinically active CD. Moreover, the CDAI score was not correlated with relapse, admission, surgery, or the need for other medications in patients with clinical remission of CD.
The new goal of treatment is no longer only clinical remission indicated by a CDAI score of <150, but also the induction and maintenance of mucosal healing.2427 Patients with both deep remission (defined as CDAI scores <150) and mucosal healing seem to have better outcomes than patients with only clinical remission or only mucosal healing.2829 Mucosal healing detected with MRE imaging was well correlated with the disease activity of CD.8 In our study, mucosal healing detected with MRE was found in only 17 (27.9%) patients with clinical remission of CD and 19 (17%) patients with clinically active CD; however, there was no statistically significant difference (P=0.091). This implies that clinical symptoms according to the CDAI score are not correlated with the actual mucosal state detected with MRE imaging. Forty-four (72.1%) patients with clinical remission assessed according to clinical symptoms had active inflammation on MRE, which suggests that many patients without symptoms might have active intestinal inflammation.
MRE is now recommended as a new diagnostic tool in the management of CD.30 MRE is a radiation-free imaging technique used to obtain cross-sectional images of the small bowel, and can describe the whole of the gastrointestinal tract, including mucosal, mural, and extramural tissues.30 Cross-sectional imaging is important in assessing diseases in parts of the small bowel that are difficult to reach by using enteroscopy.31 MRE also has a role in the detection of complications of small-bowel CD and postoperative CD recurrence.32 CD involvement of the proximal small bowel has a higher risk of stricturing behavior and the requirement for multiple surgeries.33 In our study, stricturing disease (B2) and penetrating disease (B3) according to the Montreal classification increased the risk for hospitalization by more than two times, compared with nonstricturing or nonpenetrating disease (B1) in patients with clinically active CD. Moreover, penetrating disease (B3) increased the risk for surgery by more than five times.
The current retrospective study provides evidence of the usefulness of MRE in assessing the prognosis of CD. The presence of active inflammation on MRE increased the risk (by more than six times) for relapse and the need for adding other medications or increasing the dose of current medications in patients with clinical remission of CD. Moreover, the presence of active inflammation on MRE increased the risk for CD-related admission in patients with clinically active CD.
In a recent study, the radiologic response with CTE or MRE was associated with significant reductions in the long-term risk of hospitalization, surgery, or corticosteroid use among patients with small-bowel CD, supporting our results.12 Complete radiologic response, defined as improvement of all lesions at a second imaging study, decreased the risk for steroid use and surgery by >60% and the risk for hospitalization by 70%.12 In our study, we focused on the effects of the first findings of MRE imaging at the time of clinical remission and during the clinically active state in patients with CD, separately. Moreover, we included patients with L2 disease (colonic lesion) according to the Montreal classification, and analyzed the risk of clinical relapse and the need for adding other medications or increasing the dose of current medications. In this study, the risk of surgery and need for corticosteroids were not correlated with the initial MRE findings; however, the risk for clinical relapse, hospitalization, and the need for adding other medications or increasing the dose of current medications were significantly related to the findings of active inflammation on the initial MRE study.
This study has some limitations. As this was a retrospective study with a chart review, there was a timing difference between remission or relapse and MRE imaging in each patient. MRE imaging was done during a long-standing clinical remission state in some patients, whereas other patients underwent imaging study immediately after clinical remission. We did not analyze the MRE findings with regard to mural thickening or edema because we only focused on the prognostic significance of the mucosal healing phase against active inflammation. Furthermore, MRE activity was not classified into specific degrees using previous alleged scoring systems such as magnetic resonance index of activity (MaRIA), Crohn's disease activity score (CDAS), or magnetic resonance enterography global score (MEGS). Prognosis could be affected by change of treatment options or physician's decisions, but these factors were not considered. In addition, pediatric patients <18 years old were excluded, and we were not able to analyze the effects of anti-Saccharomyces cerevisiae antibody and fecal calprotectin level because of a lack of data. Colonoscopic findings were not analyzed with MRE findings because there was a time difference between the days of colonoscopic examination and MRE imaging examination, and most patients had small-bowel involvement. Further studies about the correlation between endoscopic and MRE imaging findings are needed. In another study, high CRP at the time of CD diagnosis was risk factor for hospitalization;34 however, we were not able to find a relationship between CRP level and prognosis. This report is the first study to evaluate the clinical outcomes of findings of active inflammation on MRE imaging in patients with CD.
In conclusion, the presence of active inflammation on MRE in patients with CD at the time of clinical remission was significantly associated with a high risk of relapse and the need for adding other medications or increasing the dose of current medications. Moreover, the presence of active inflammation during the clinically active state was significantly associated with an increased risk of hospitalization. MRE might be a useful technique in monitoring disease activity in patients with CD.
Notes
FINANCIAL SUPPORT: This research was supported by two grants (A120176, HI13C1345) from the Korean Health Technology R&D Project through the Korea Health Industry Development Institute, which is funded by the Ministry of Health and Welfare, Republic of Korea, and two grants (NRF-2013R1A2A2A01067123, NRF-2014R1A1A1008096) from the Basic Science Research Program through the National Research Foundation of Korea, which is funded by the Ministry of Science, ICT and Future Planning.
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION: Guarantor of the article: Jae Hee Cheon and Joon Seok Lim.
Specific author contributions: Ji Hoon Lee: acquisition of data; analysis and interpretation of data; drafting of the manuscript. Yong Eun Park: acquisition of data; study concept and design. Nieun Seo: acquisition of data; study concept and design. Hyun Jung Lee: acquisition of data; study concept and design. Soo Jung Park: study concept and design; critical revision of the manuscript for important intellectual content. Tae Il Kim: study concept and design; critical revision of the manuscript for important intellectual content. Won Ho Kim: study concept and design; critical revision of the manuscript for important intellectual content. Jae Hee Cheon and Joon Seok Lim: acquisition of data; study concept and design; critical revision of the manuscript for important intellectual content. All authors approved the final version of the article, including the authorship list.




