INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic and relapsing inflammatory disorder of the intestine with an interplay of genetic, immunological, and environmental factors with intestinal microbes. IBD is categorized into 2 identified subtypes: Crohnâs disease (CD) and ulcerative colitis (UC) [1]. The disease course of IBD can wax and wane over time, and the spectrum of severity, including stricturing, penetrating complications, and colitis-associated malignancies, is wide [2]. Understanding the epidemiology and disease burden of this incurable, lifelong disease is crucial for better management of patients and allocation of health care resources. Traditionally, IBD has been known as a disease of Caucasians in the industrialized regions of the Western world [3]. However, the incidence of IBD has increased in the newly industrialized regions such as Asia, while industrialization has increased in these areas since the late 20th century [2,3]. Data on the epidemiology of IBD in Asia have been scarce and heterogeneous with conflicting findings [4]. Therefore, in this review, recent updated data regarding the incidence and prevalence of IBD in Asia are discussed to understand the epidemiologic status and disease burden of this area with a huge population.
RECENT UPDATE ON THE EPIDEMIOLOGY OF IBD IN ASIA
In Asian countries, data on the longitudinal analyses of population-based studies on the incidence and prevalence of IBD have been insufficient. Because detailed and systematic review articles on similar issues have been published recently [3,5,6], we tried to search and update the most recent data on the epidemiology of IBD in Asian countries, which have been published within 3 to 5 years.
1. Incidence
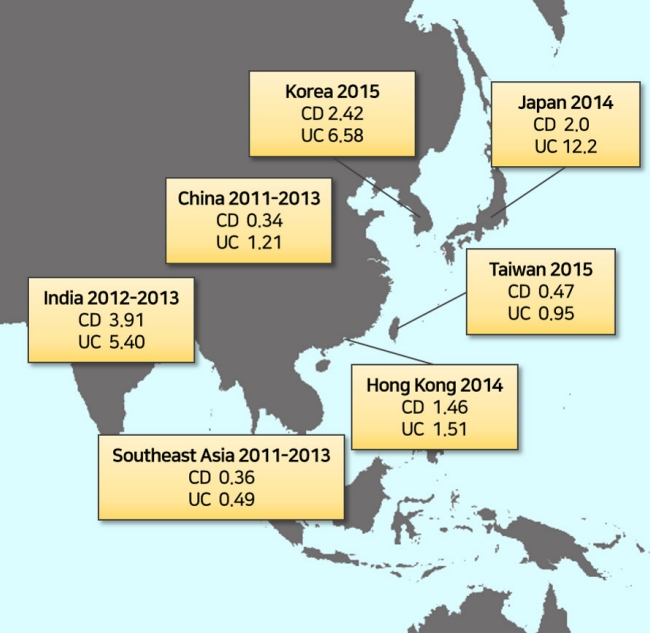
The most recent data on the incidence of IBD in Asian countries were shown in Fig. 1. Recently, the incidence and prevalence of IBD in a population-based inception cohort from Songpa-Kangdong district, Korea was updated with a 30-year study period from 1986 to 2015 [7]. The age- and sex-adjusted annual incidence of IBD has increased continuously throughout the 30-year period: from 0 in 1986 to 2.42/100,000 inhabitants in 2015 for CD and from 0.33/100,000 inhabitants in 1986 to 6.58/100,000 inhabitants in 2015 for UC. According to this study, CD incidence had increased approximately 40 times during the past three decades, and UC incidence had increased approximately 20 times. The average annual percentage change (APC) in IBD incidence was 12.3% during 1986-1995 and 12.3% during 1996-2005, whereas it was only 3.3% during 2006-2015 (P< 0.05). This indicates a moderation in the increase in IBD incidence in recent years, despite the continued increase in the incidence of IBD. Recently, the incidence and prevalence data from Korea using a nationwide health insurance database reported conflicting results [8-10]. Two studies reported a plateau or even decrease in the IBD incidence in Korea between 2006 and 2014 [8,9]. One of the studies reported CD and UC incidences as 3.6/100,000 and 5.0/100,000, respectively, in 2006 and 3.1/100,000 and 4.2/100,000, respectively, in 2012 [8]. The other study reported the incidences of CD and UC as 3.1/100,000 and 5.9/100,000, respectively, in 2011 and 2.4/100,000 and 5.0/100,000, respectively, in 2014 [9]. However, the most recent study using this database reported of increased IBD incidence between 2009 and 2016 [10]. This study reported the incidences of CD and UC as 2.4/100,000 and 4.0/100,000, respectively, in 2009 and 2.9/100,000 and 4.0/100,000, respectively, in 2016 [10]. This discrepancy could be because of the difference in the definition of incident cases and relatively short washout periods between the enrollment in the administrative database and IBD diagnosis, which can cause a misclassification between the incident and prevalent cases [11]. A similar discrepancy was observed for North America in which the incidence of IBD decreased between 1996 and 2009 in the Canadian population-based study [12]. Cases may have been underestimated because IBD diagnosis was not based on clinical diagnosis and medical record review, but on a diagnostic code-based scoring systems including the International Classification of Diseases-9 codes, physician billing claims, and discharge diagnoses [2,11].
In 2019, longitudinal data on the incidence of IBD were reported in Taiwan [13]. A retrospective analysis was performed using data, between January 2001 and December 2015, from the National Health Insurance and the Ministry of Health and Welfare, Taiwan. The crude incidence of CD increased from 0.17/100,000 in 2001 to 0.47/100,000 in 2015, and the crude incidence of UC increased from 0.54/100,000 in 2001 to 0.95/100,000 in 2015. The APC was 2.69 by the joinpoint trend analysis for the general trends in patients diagnosed with IBD, which was significant from 2001 to 2015. The trend of CD also increased significantly according to the joinpoint trend analysis from 2001 to 2015, with the APCs as 4.75 (2001-2010) and 15.92 (2010-2015), whereas they were nonsignificant in the trend for UC, given that the APC value was 0.82 from 2001 to 2015.
According to the multinational epidemiological study from Asia, the Asia-Pacific Crohnâs and Colitis Epidemiologic Study (ACCESS), the incidence of IBD had an increasing trend in Asian countries including Brunei, China, Hong Kong, India, Indonesia, Macau, Malaysia, Singapore, Sri Lanka, Taiwan, Thailand, and the Phillippines [4,14]. Between 2011 and 2013, the mean annual crude incidence of IBD per 100,000 in Asia was 1.50 (95% confidence interval [CI], 1.43-1.57). From 2011 to 2012, the crude overall annual incidence per 100,000 of IBD, CD, and UC in Asia was 1.14 (95% CI, 1.06-1.23), 0.35 (95% CI, 0.31-0.40), and 0.76 (95% CI, 0.69-0.84), respectively. From 2012 to 2013, and the corresponding incidence rates were 1.89 (95% CI, 1.77-2.01), 0.66 (95% CI, 0.60-0.73), and 1.20 (95% CI, 1.11-1.29), respectively.
In a multicenter study using a hospital and territory-wide administrative coding system from Hong Kong, the age-adjusted incidence of IBD per 100,000 individuals increased from 0.10 (95% CI, 0.06-0.16) in 1985 to 3.12 (95% CI, 2.88-3.38) in 2014 [15]. The age-adjusted incidence per 100,000 increased from 0.01 (95% CI, 0.00-0.05) in 1985 to 1.46 (95% CI, 1.29-1.65) in 2014 for CD and from 0.09 (95% CI, 0.05-0.15) in 1985 to 1.51 (95% CI, 1.35-1.69) in 2014 for UC.
In Japan, recent data on the longitudinal analysis of IBD epidemiology have been lacking. However, we have observed a constant increase in the incidence of IBD over the past 60 years, as published in the previous reports. In 1955, the incidence of CD and UC was 0.002/100,000 and 0.03/100,000, respectively [16]. In 1991, the incidence of CD and UC had risen to 0.51/100,000 and 1.95/100,000, respectively [17]. From 1986 to 1998, the CD incidence has been estimated to be as high as 0.9/100,000 [18]. A recent report using a survey conducted in 2014 reported the incidence of CD as 2.0/100,000 and the incidence of UC as 12.2/100,000 [19].
In China, longitudinal data on the trend in the incidence of IBD is not available. In meta-analyses that summarized the epidemiologic data on a national level, the incidence of CD was estimated at 0.28/100,000 during 1950-2002 and this was slightly increased to 0.85/100,000 on extending the period to 1950-2007 in mainland China [20,21]. A population-based study from Wuhan reported the age-adjusted incidence of IBD, CD, and UC were 1.96, 0.51, and 1.45/100,000, respectively [22]. According to ACCESS, the pooled incidence rates of IBD, CD, and UC in China were 1.61, 0.34, and 1.21, respectively, between 2011 and 2013 [14]. In addition, within China, the pooled incidence of IBD varied from 0.18/100,000 to 0.73/100,000 for CD and 1.12/100,000 to 1.33/100,000 for UC according to the population density of the regions [14].
In Southeast Asia and South Asia, only a few studies on the epidemiology or natural course of IBD have been published [23-27], most of which are referral-center-based studies. Based on the data from the ACCESS, the pooled incidence of UC was lower in Southeast Asia than that in East Asia (0.49/100,000 vs. 1.14/100,000; P= 0.002) and the pooled incidence of CD was comparable between Southeast Asia and East Asia (0.36/100,000 vs. 0.34/100,000; P= 0.878) [14]. In Malaysia, the first population-based study from the Kinta Valley region reported the incidence of IBD as steadily increased over the past two decades; from 0.07/100,000 population-years in 1990-1995 to 0.69/100,000 population-years in 2005-2010 [26]. In a Malaysian hospital-based study, the mean crude incidence of IBD had increased steadily between 1980 and 2018: 0.36 (1980-1989), 0.48 (1990-1999), and 0.63/100,000 person-years (2000-2009). From 2010 to 2018, the mean crude incidence doubled to 1.46/100,000 person-years [28]. In the ACCESS, India showed a higher incidence of IBD than those of East Asia and Southeast Asia (9.31/100,000 vs. 1.53/100,000 and 0.80/100,000) [14].
2. Prevalence and Estimated Number of Patients with IBD
Table 1 lists the recent prevalence data from the Asian countries. We calculated the actual number of patients with IBD to estimate the real disease burden of IBD in this region. Census data from each country were used to estimate the national population for the years of the prevalence study. Available data on prevalence were superimposed on the national population at the time of the study to estimate the disease burden of CD or UC. In Korea and Japan, approximately 0.1%-0.2% of the general population may have IBD [7,19]. This range is lower than that in the Western regions such as the United States, affecting up to 0.5% of the general population [31,32,34]. Taiwan, Hong Kong, and Malaysia have a lower IBD disease burden than that of Korea and Japan [13,15,26]. Although no recent prevalence data have been reported in China and India, which have a huge population of more than 1 billion people, these countries might have substantially higher numbers of patients with IBD compared Western countries [35]. In Central Asia, one recent report on the prevalence of IBD in Kazakhstan showed that the prevalence of IBD, CD, and UC were 113.9/100,000, 29.5/100,000, 84.4/100,000 without incidence data [30]. However, these figures are much higher than that reported by the Ministry of Health of Kazakhstan (31.5/100,000 for UC and 6.3/100,000 for CD), maybe because of the heterogeneity of study designs [36].
DISCUSSION
Kaplan and Windsor [37] had recently suggested that the evolution of IBD epidemiology can be stratified into 4 epidemiological stages: emergence (sporadic incident cases with IBD begin to emerge in a population), acceleration in incidence (a dramatic increase in the number of incident cases with IBD is observed, but overall prevalence remains low), compounding prevalence (incidence rates of IBD stabilize or even decline, but the slope of prevalence of IBD continues to accelerate owing to decades of high incidence with low mortality), and prevalence equilibrium (the slope of prevalence of IBD begins to level off owing to stable incidence of IBD and an aging prevalent population with higher mortality). Based on this stratification, most Asian countries experiencing a rising incidence with a low prevalence of IBD are embedded in the second epidemiological stage (acceleration in incidence). Considering the huge population in Asian countries, including China and India, Asia alone might have a greater disease burden with IBD than that of the Western world in the near future. One modeling study from Iran expected a 1.5-fold increase in prevalence for East Asia with 4.5 million cases of IBD and quadrupling of the prevalence for India with 2.2 million cases of IBD in 2035, as compared to 2020 [38]. However, data should be interpreted with caution given the vast heterogeneity between the reported incidence rates among the Asian countries and regions within these countries, such as data of the ACCESS [4,30,36,37]. Asian countries are currently in various stages according to the industrialization status. For example, Korea and Japan have experienced more rapid industrialization than the other Asian countries and transitioned into the second stage earlier than the other Asian countries. Therefore, these countries may enter the compounding prevalence stage (stage 3) with a rapid increase in the prevalence of IBD after several decades of accelerated incidence (stage 2), similar to the experience in Western countries in the 21st century. In conclusion, considering the current status of rapidly rising incidence and the subsequent explosive increase in the prevalence of IBD in Asia, the healthcare delivery systems, including the resource setting, should be prepared for this challenge by understanding the exact disease burden of IBD in this region.